Abducens Neurovascular Conflict¶
Summary
- Vascular compression of the sixth cranial nerve causing diplopia due to lateral rectus palsy
- Results from arterial loop compression at the nerve root exit zone or cisternal segment
- MRI with high-resolution T2-weighted sequences demonstrates vascular contact with nerve displacement or distortion
Pathophysiology¶
- Direct pulsatile compression of CN VI by adjacent vessel causes demyelination and axonal injury
- Most common offending vessels:
- Anterior inferior cerebellar artery (AICA)
- Basilar artery
- Vertebral artery
- Superior cerebellar artery (SCA)
- Compression typically occurs at:
- Root exit zone (REZ) at pontomedullary junction
- Cisternal segment within prepontine cistern
- Chronic pulsatile trauma leads to:
- Focal demyelination
- Ephaptic transmission
- Hyperexcitability of nerve fibres
Demographics¶
- Rare condition with limited epidemiologic data
- Age distribution:
- Most common in adults 40-70 years
- Can occur at any age
- No significant gender predilection
- Often unilateral, bilateral cases are rare
- Associated conditions:
- Hypertension (may contribute to vessel tortuosity)
- Atherosclerosis
- Vertebrobasilar dolichoectasia
Diagnosis¶
- Clinical presentation:
- Horizontal diplopia worse on lateral gaze
- Esotropia of affected eye
- Inability to abduct affected eye
- No associated cranial nerve deficits
- Differential diagnosis:
- Microvascular ischaemia (diabetic sixth nerve palsy)
- Increased intracranial pressure
- Cavernous sinus pathology
- Posterior fossa tumours
- Wernicke encephalopathy
- Multiple sclerosis
- Diagnostic criteria:
- Clinical evidence of sixth nerve palsy
- MRI demonstration of neurovascular contact
- Exclusion of other causes
Imaging¶
-
MRI Protocol:
- High-resolution 3D sequences essential
- Thin-slice acquisitions (≤1mm)
-
T2:
- 3D CISS/FIESTA/DRIVE sequences optimal
- Hyperintense CSF provides excellent contrast
- Demonstrates nerve-vessel contact point
- May show nerve displacement or indentation
-
T1:
- Hypointense nerve against intermediate signal CSF
- Less optimal for neurovascular relationships
-
T1+C:
- Usually not indicated
- May help exclude enhancement from inflammatory causes
- Vessels show flow voids or enhancement
-
DWI:
- Typically normal
- Excludes acute ischaemic changes
-
SWI:
- Demonstrates vascular structures as signal voids
- Helps differentiate vessels from other structures
- May show venous structures if involved
-
MRA:
- TOF-MRA or contrast-enhanced MRA
- Identifies offending vessel anatomy
- Demonstrates vascular loops or ectasia
- Useful for surgical planning
-
Additional findings:
- Nerve atrophy in chronic cases
- Vessel loop configuration at compression site
- Distance from REZ to compression point
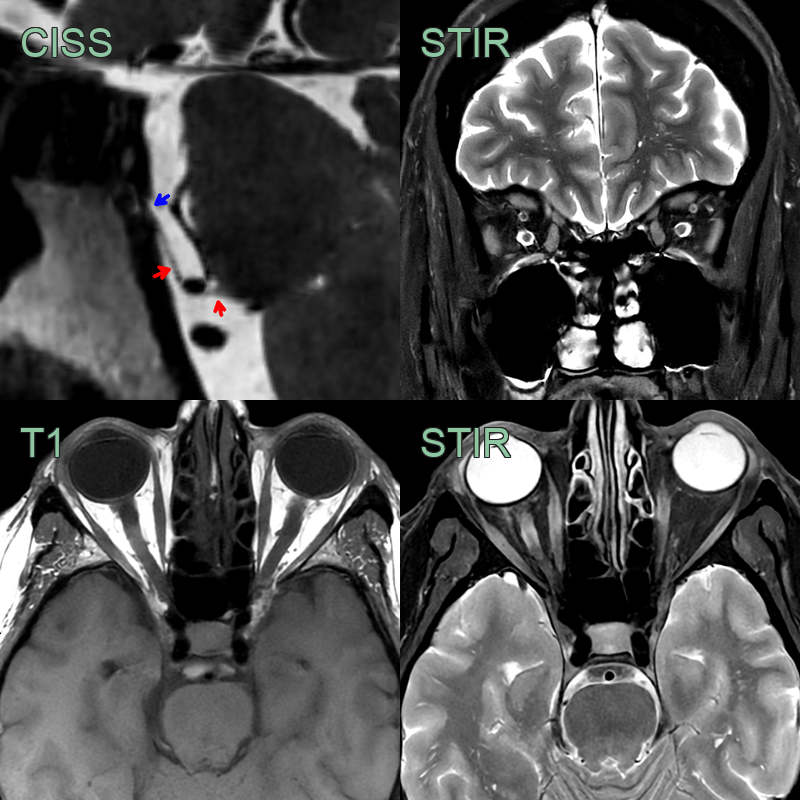
- A 40-year-old patient presented with a progressive left abducens palsy.
- MRI showed the cisternal segment of the abducens nerve (red) distorted by the AICA before entering Dorello's canal.
- The left lateral rectus muscle was subtly T2-hyperintense and atrophic.
Treatment¶
-
Conservative management:
- First-line for most patients
- Observation for 3-6 months (spontaneous resolution possible)
- Prism glasses for symptomatic relief
- Botulinum toxin injection to medial rectus
-
Medical therapy:
- Carbamazepine or gabapentin (limited efficacy)
- Treatment of underlying vascular risk factors
- Blood pressure control
-
Surgical intervention:
- Microvascular decompression (MVD)
- Indicated for persistent, disabling symptoms
- Retrosigmoid or subtemporal approach
- Teflon felt placement between nerve and vessel
- Success rate approximately 70-80%
- Risks:
- Hearing loss
- CSF leak
- Meningitis
- Stroke
- Incomplete symptom resolution
-
Outcomes:
Differential diagnosis¶
| Differential diagnosis for a 6th nerve palsy | Differentiating feature |
|---|---|
| Abducens nerve schwannoma | MRI shows enhancing mass along CN VI course; progressive symptoms rather than episodic spasms |
| Increased intracranial pressure | Bilateral sixth nerve palsies; papilledema on fundoscopy |
| Cavernous sinus thrombosis | Associated with fever, proptosis, chemosis, and involvement of CN III, IV, V1, V2 |
| Gradenigo syndrome | Associated with otitis media/mastoiditis; facial pain in V1 distribution; otorrhea |
| Multiple sclerosis | Multiple white matter lesions on MRI; oligoclonal bands in CSF |
| Thyroid eye disease | Proptosis, lid retraction, restrictive myopathy on forced duction testing |
| Dorello's canal meningioma | Enhancing dural-based mass in Dorello's canal on MRI |
| Petrous apex lesion | Bone erosion or mass lesion at petrous apex on CT/MRI |
| Microvascular ischaemia | Age >50, vascular risk factors; spontaneous recovery; no vascular loop on MRI |