Acquired Hepatocerebral Degeneration¶
Summary
- Neurological syndrome characterised by extrapyramidal and neuropsychiatric symptoms
- Occurs in patients with chronic liver disease and portosystemic shunting
- MRI shows T1 hyperintensity in basal ganglia, particularly globus pallidus
Pathophysiology¶
- Accumulation of manganese in basal ganglia due to impaired liver function
- Astrocyte alterations (Alzheimer type II astrocytes) in basal ganglia and cerebral cortex
- Oxidative stress and mitochondrial dysfunction contribute to neuronal damage
Demographics¶
- Affects 1-2% of patients with cirrhosis
- More common in males (2:1 male to female ratio)
- Typically occurs in middle-aged to older adults with long-standing liver disease
Diagnosis¶
- Clinical presentation:
- Extrapyramidal symptoms: tremor, bradykinesia, rigidity
- Neuropsychiatric symptoms: cognitive impairment, personality changes
- Ataxia and dysarthria
- Laboratory findings:
- Elevated serum ammonia levels
- Abnormal liver function tests
- Exclusion of other causes of neurological symptoms in cirrhosis (e.g., Wernicke's encephalopathy)
Imaging¶
- MRI findings:
- T1 hyperintensity in basal ganglia, particularly globus pallidus
- Symmetric involvement of caudate nucleus, putamen, and subthalamic nuclei
- Normal signal on T2-weighted and FLAIR sequences
- CT:
- May show hyperdensity in basal ganglia, but less sensitive than MRI
- PET:
- Decreased glucose metabolism in basal ganglia and cerebral cortex
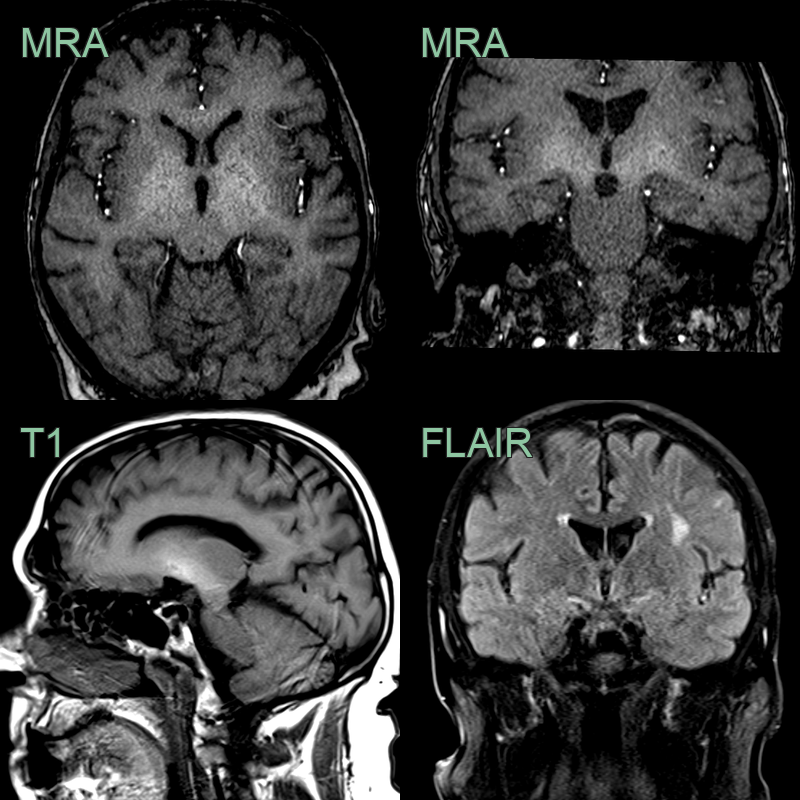
- In a patient with alcoholic liver disease, there is symmetrical T1-hyperintensity in the globi pallidi and subganglionic region.
Treatment¶
- Management of underlying liver disease:
- Treatment of hepatic encephalopathy
- Consideration of liver transplantation in appropriate candidates
- Symptomatic treatment:
- Levodopa for parkinsonian symptoms (limited efficacy)
- Trientine or penicillamine for manganese chelation (experimental)
- Supportive care:
- Physical therapy and occupational therapy
- Management of neuropsychiatric symptoms
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Wilson's Disease | Younger age of onset, Kayser-Fleischer rings, low serum ceruloplasmin |
| Hepatic Encephalopathy | More acute onset, fluctuating course, asterixis, responds to ammonia-lowering therapies |
| Manganese Toxicity | Symmetrical T1 hyperintensity of globi pallidi and subthalamic nuclei; imaging indistinguishable without history |
| Pantothenate Kinase-Associated Neurodegeneration (PKAN) | "Eye of the tiger" sign — T2 hypointensity in globus pallidus with central hyperintensity |
| Multiple System Atrophy | Autonomic dysfunction, cerebellar signs, poor response to levodopa |
| Leigh Syndrome | Earlier onset, brainstem and basal ganglia lesions on MRI, metabolic acidosis |
| Carbon Monoxide Poisoning | History of exposure, globus pallidus lesions on MRI |