Acute Ischaemic Stroke¶
Summary
- Acute ischaemic stroke is characterised by sudden onset neurological deficits due to focal brain ischaemia
- Caused by thrombotic or embolic occlusion of cerebral arteries
- Rapid diagnosis and treatment are crucial for improved outcomes
Pathophysiology¶
- Interruption of blood flow to brain tissue leads to:
- Rapid depletion of oxygen and glucose
- Failure of cellular energy metabolism
- Ionic pump dysfunction and excitotoxicity
- Cell death in the ischaemic core
- Penumbra: potentially salvageable tissue surrounding the ischaemic core
- Time-dependent progression of irreversible damage without reperfusion
Demographics¶
- Risk factors:
- Age: incidence doubles each decade after 55 years
- Gender: higher incidence in men, but more severe in women
- Race: higher risk in African Americans and Hispanics
- Modifiable factors: hypertension, diabetes, smoking, obesity, atrial fibrillation
Diagnosis¶
- Clinical presentation:
- Sudden onset of focal neurological deficits
- Common symptoms: hemiparesis, aphasia, visual disturbances, ataxia
- Initial assessment:
- National Institutes of Health Stroke Scale (NIHSS)
- Blood tests: glucose, coagulation profile, complete blood count
- ECG to detect atrial fibrillation
- Time is critical: "Time is Brain" concept
Imaging¶
- Non-contrast CT:
- First-line imaging modality
- Excludes haemorrhage and large established infarcts
- Early ischaemic changes: loss of gray-white differentiation, hyperdense vessel sign
- CT angiography:
- Identifies site of vessel occlusion
- Evaluates collateral circulation
- CT perfusion:
- Assesses cerebral blood flow, volume, and mean transit time
- Helps identify penumbra and guide treatment decisions
- MRI:
- Higher sensitivity for early ischaemic changes
- Diffusion-weighted imaging (DWI) shows restricted diffusion in acute infarcts
- Perfusion-weighted imaging (PWI) identifies penumbra
- DWI-PWI mismatch guides treatment in extended time windows
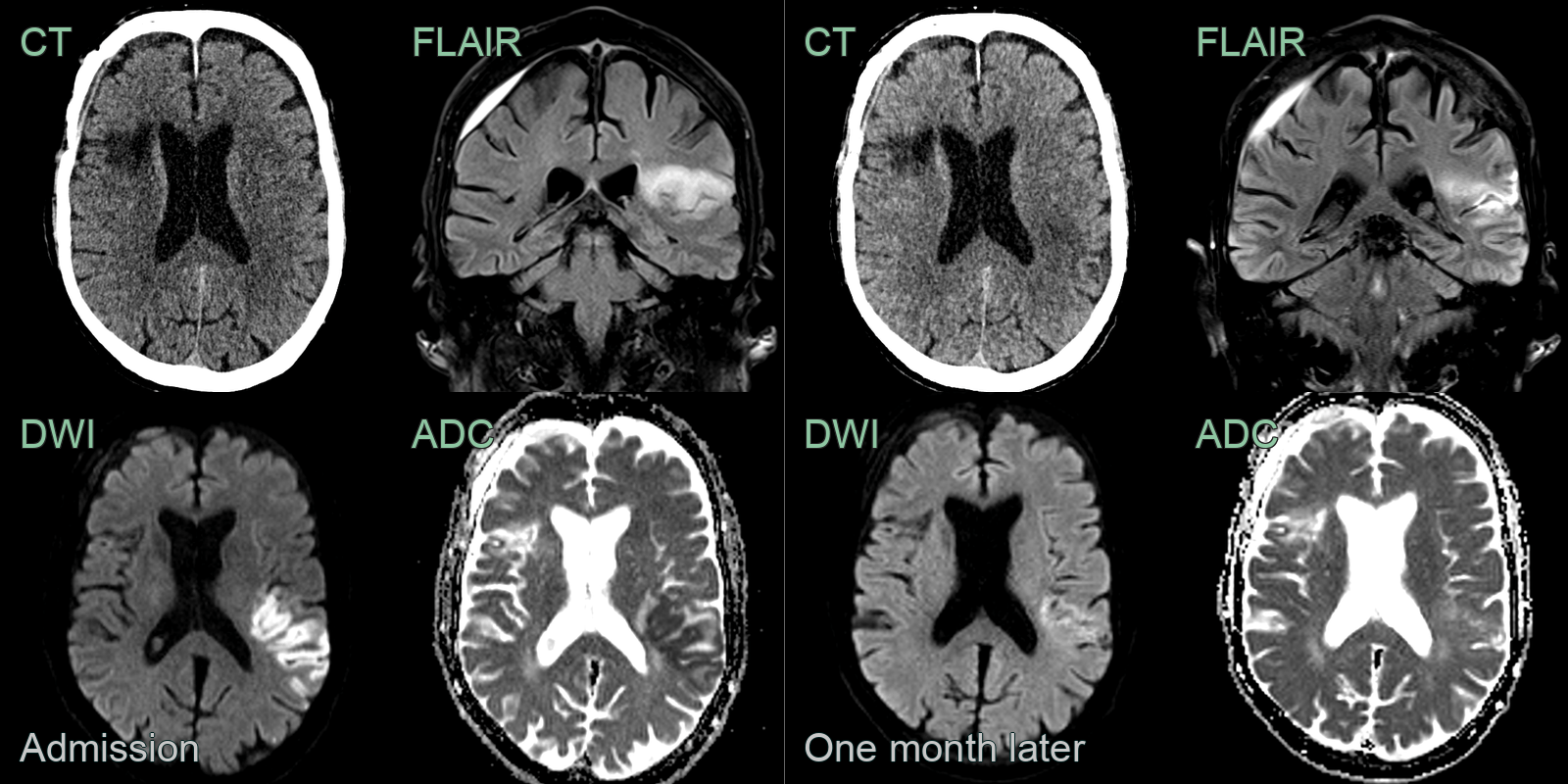
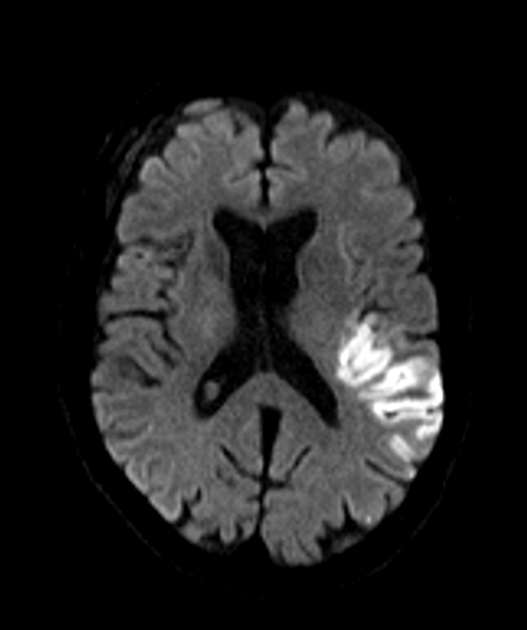
- A 70-year-old patient presenting with right sided weakness and dysarthria.
- At presentation, there was very subtle loss of grey-white matter differentiation on CT. On MRI, high DWI signal corresponded to low values on the ADC map.
- 1 month later, the DWI hyperintensity had regressed and the ADC values had increased.
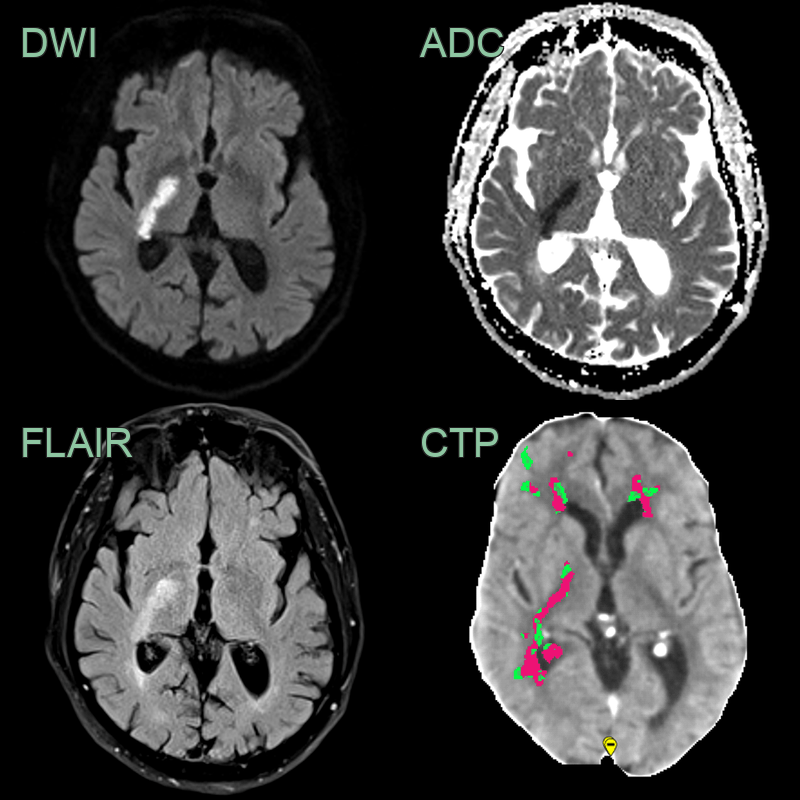
- A 65-year-old patient presenting with left sided weakness.
- DWI shows an acute infarct selectively involving the posterior limb of the internal capsule representing the territory of the anterior choroidal artery.
- While there was no abnormality on the CT, on hindsight, there was a region of abnormal perfusion (reduced CBF and increased Tmax) on the CTP performed the day prior.
- A 70-year-old patient present with a mixed sensory and motor deficit. While the NCCT did not convincing acute infarct, the CTA showed an area of hypoenhancement in the anterior thalamus. An acute thalamic infarct was confirmed on DWI.
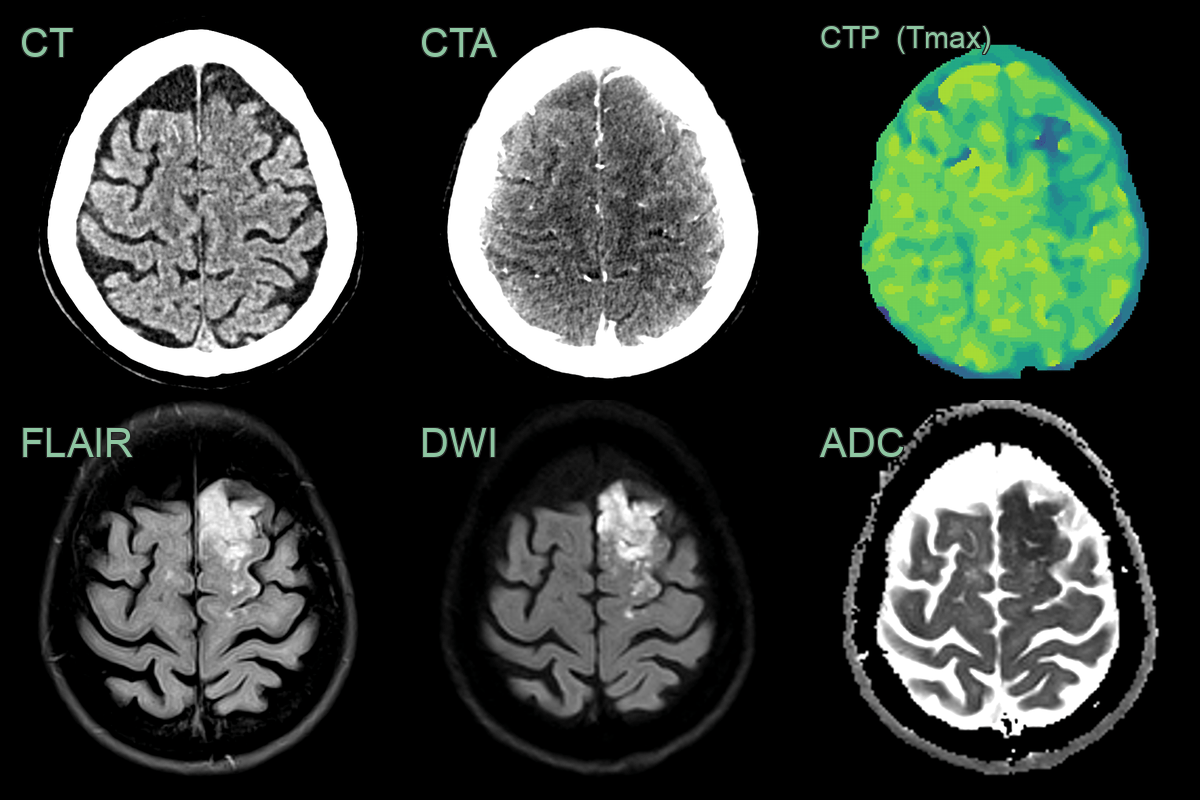
- A 60-year-old patient presented with aphasia and difficulty walking.
- CT showed a subtle region of cortical hypodensity in the left superior frontal gyrus (corresponding to the left ACA territory).
- CTA showed cortical hypoenhancement.
- CTP showed a prolonged Tmax (and decreased CBF and CBV).
- MRI showed high FLAIR signal and diffusion restriction (hyperintensity on B1000 DWI images corresponding to low values on the ADC map).
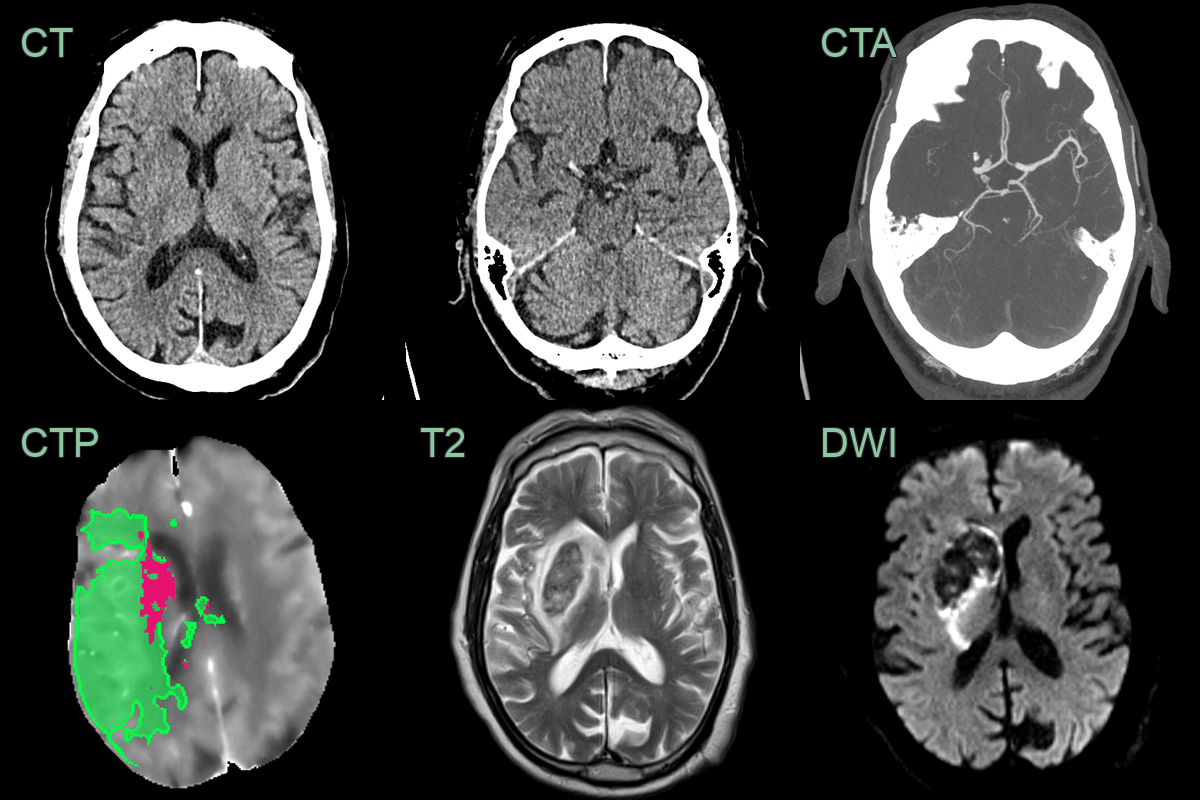
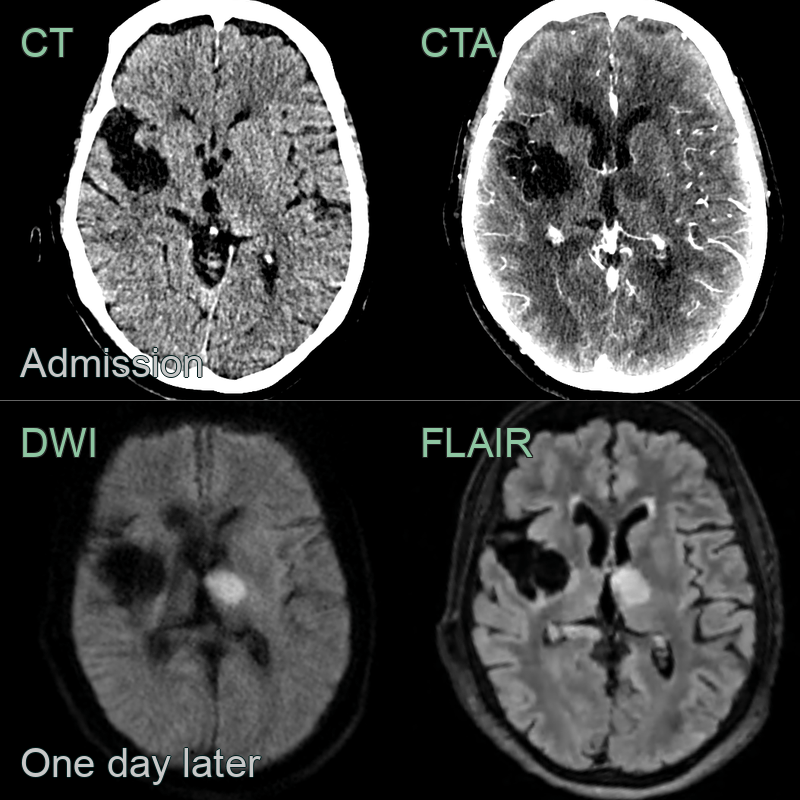
- A 80-year-old patient presented with a dense left sided weakness.
- CT showed a subtle area of acute ischaemia in the rigth caudate head.
- CTA showed a proximal occlusion of the right MCA.
- CTP showed a large penumbra and small core infarct.
- MRI performed 1 day after a mechnical thrombectomy showed no iscaehmic damage in the penumbra (and haemorrhagic transformation in the area of core infarction).
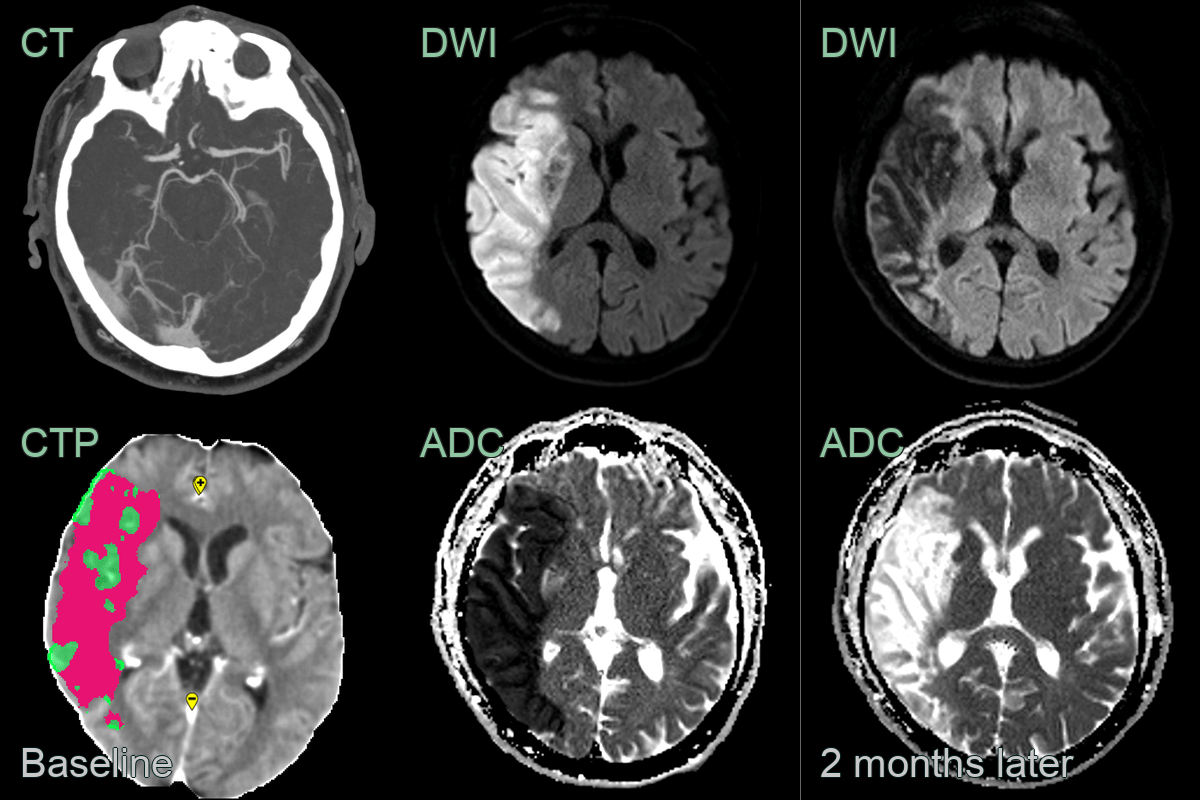
- A patient presented with a dense left sided hemiplegia.
- CTA showed a mid-M1 MCA occlusion. CTP showed a large core infarct (pink) with no sizeable penumbra (green).
- The diffusion restriction at baseline was replaced by facilitated diffusion due to encephalomalacia after 2 months.
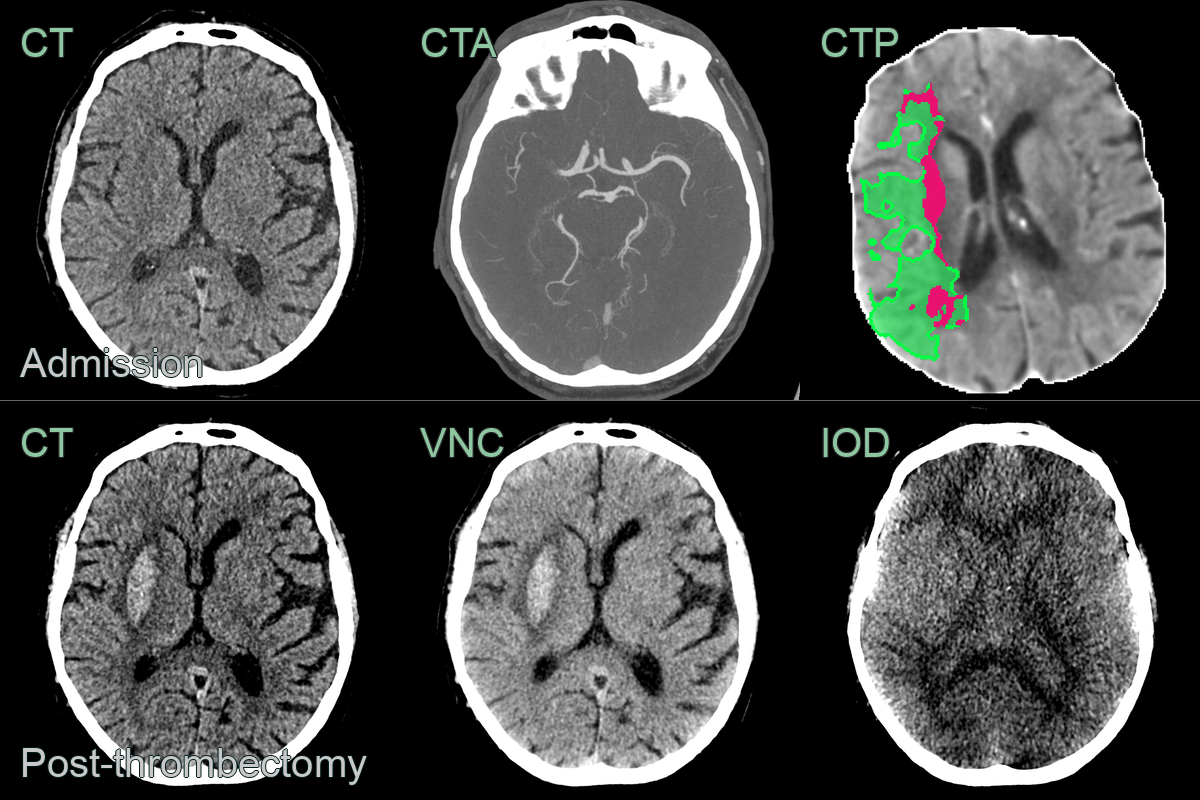
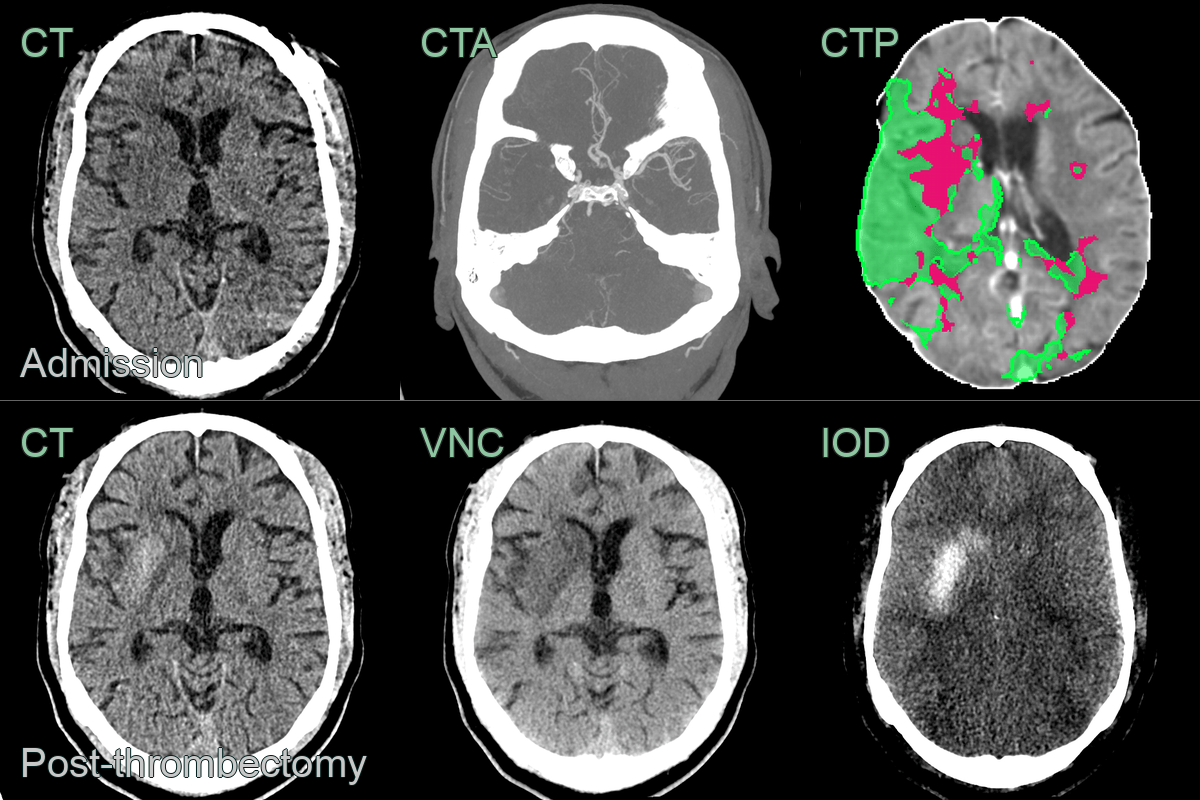
- A 70-year-old patient presented with a dense left-sided weakess.
- Imaging showed a right M1 MCA occlusion causing acute infarction (ASPECTS 8) associated with a large penumbra.
- Following a successful thrombectomy, the CT showed hyperdensity on CT. Using dual energy CT, the virtual non-contrast (VNC) showed hyperdensity in the right putamen that was not absent on the iodine map, consistent with petechial haemorrhage (as opposed to iodine staining where the inverse would have been true).
- A 50-year-old patient presented with left sided weakness secondary to a right M1 MCA occlusion.
- Contrary to the previous case, the hyperdensity in the right putamen was present on the iodine map but not the virtual non-contrast, which was consistent with iodine staining.
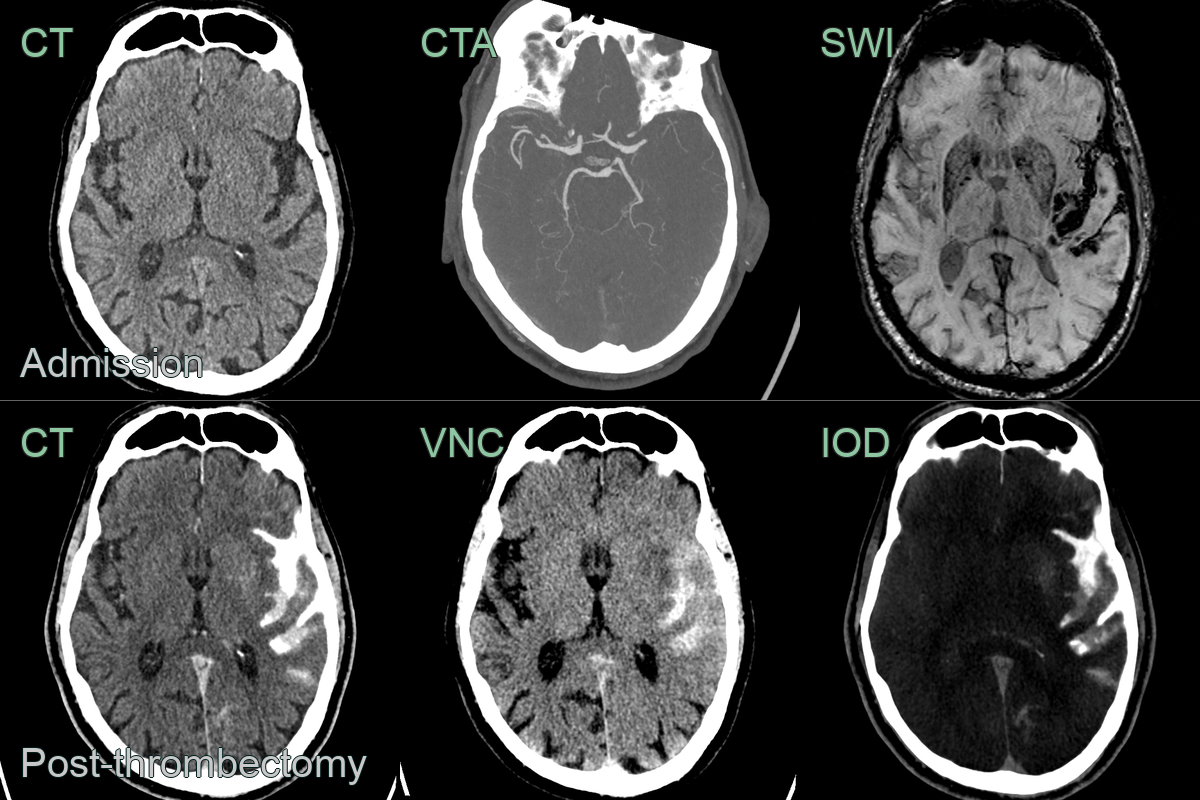
- A 65-year-old patient presented with dysphasia and right sided weakness secondary to an occluded left M1 MCA.
- Post-thrombectomy, high attenuation in the subarachnoid space was due to a combination of subarachnoid haemorrhage and seepage of iodinated contrast.
Treatment¶
- Intravenous thrombolysis:
- Recombinant tissue plasminogen activator (rtPA)
- Time window: within 4.5 hours of symptom onset
- Contraindications: recent surgery, active bleeding, anticoagulation
- Mechanical thrombectomy:
- For large vessel occlusions
- Time window: up to 24 hours in selected patients based on imaging
- Improves functional outcomes when combined with IV thrombolysis
- Supportive care:
- Blood pressure management
- Glucose control
- Temperature regulation
- Early rehabilitation
- Secondary prevention:
- Antiplatelet therapy
- Statins
- Management of risk factors (hypertension, diabetes, smoking cessation)
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| HSV encephalitis | May cross arterial territories |