Adult Onset Alexander's Disease¶
Summary
- Rare leukodystrophy characterised by progressive neurological deterioration
- Caused by mutations in the GFAP gene, leading to astrocyte dysfunction
- Typical MRI findings include atrophy and white matter abnormalities in the brainstem and cerebellum
Pathophysiology¶
- Caused by mutations in the glial fibrillary acidic protein (GFAP) gene
- Leads to accumulation of Rosenthal fibres in astrocytes
- Results in progressive demyelination and neurodegeneration
- Astrocyte dysfunction impairs blood-brain barrier integrity and neurotransmitter homeostasis
Demographics¶
- Adult-onset form typically presents after age 20
- Rare disease with an estimated prevalence of 1 in 2.7 million
- No significant gender predilection
- Most cases are sporadic, but autosomal dominant inheritance has been reported
Diagnosis¶
- Based on clinical presentation, imaging findings, and genetic testing
- Clinical features may include:
- Bulbar symptoms (dysarthria, dysphagia)
- Pyramidal signs
- Cerebellar ataxia
- Palatal myoclonus
- Genetic testing for GFAP mutations is confirmatory
- Brain biopsy (rarely performed) may show Rosenthal fibres
Imaging¶
- MRI is the imaging modality of choice
- Characteristic findings include:
- Atrophy of the medulla oblongata and upper cervical spinal cord
- Periventricular white matter abnormalities
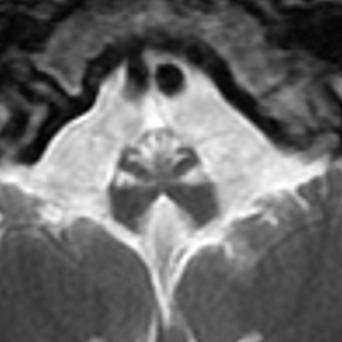
- T2 hyperintensities in the hilum of the dentate nucleus
- "Tadpole" appearance of the brainstem and spinal cord
- Advanced MRI techniques:
- Diffusion tensor imaging may show reduced fractional anisotropy in affected white matter
- MR spectroscopy may demonstrate reduced N-acetylaspartate and elevated myo-inositol
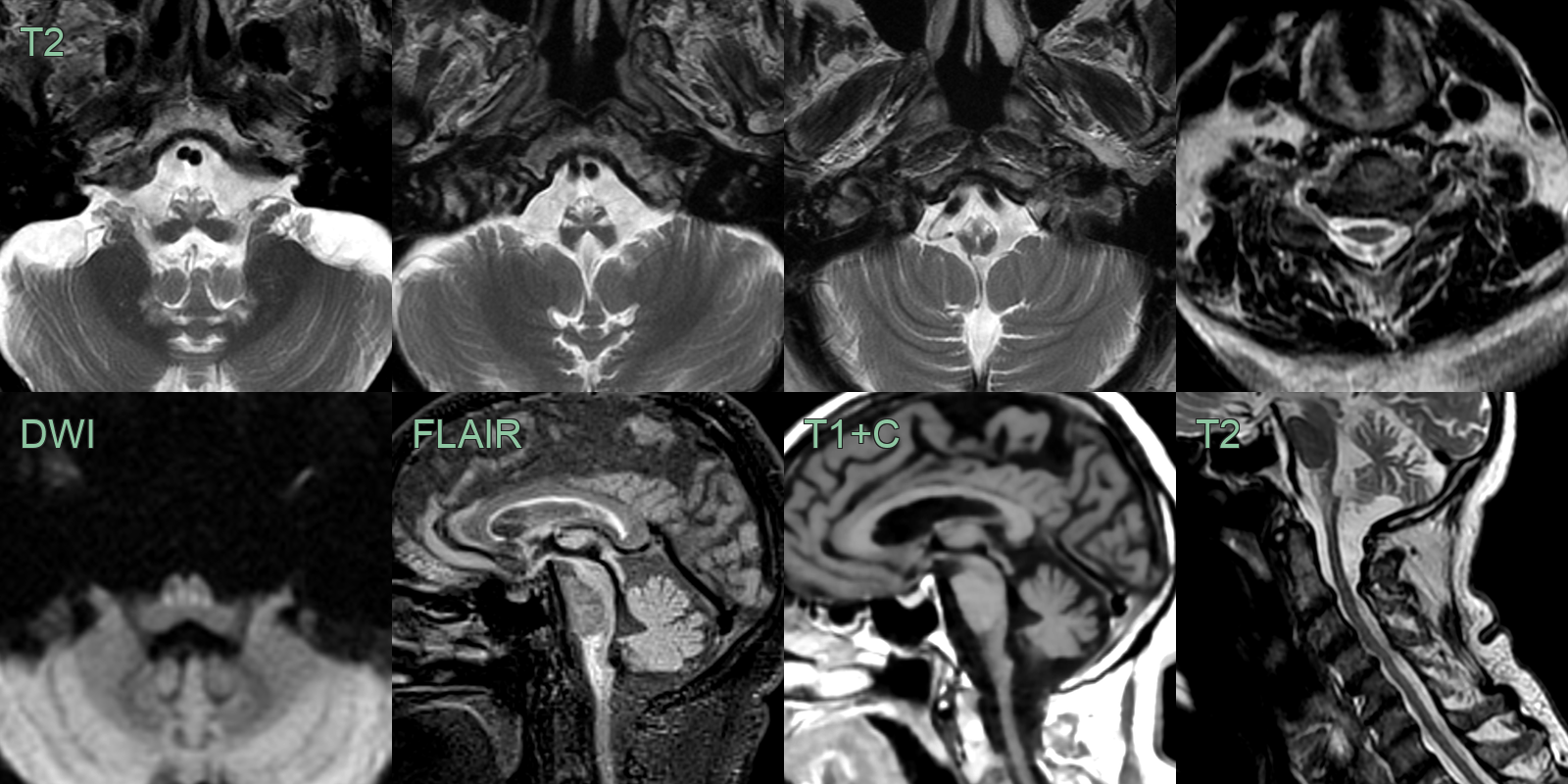
- A 50-year-old patient presented a 1 year history of progressive upper limb weakness and bulbar symptoms.
- MRI showed well demarcated symmetrical linear hyperintensity within the medulla without enhancement.
- Brainstem and cord volume loss against preserved pontine volume gives rise to the 'tadpole' sign.
Treatment¶
- No curative treatment available
- Management is supportive and symptomatic:
- Physical therapy for mobility and balance
- Speech therapy for dysarthria and dysphagia
- Antispasmodics for spasticity
- Anticonvulsants for seizures (if present)
- Experimental treatments under investigation:
- Gene therapy approaches targeting GFAP
- Small molecule therapies to reduce GFAP aggregation
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Ovoid periventricular and callosal lesions; no frontal-predominant white matter signal change or medullary involvement |
| Leukodystrophy (other types) | Different white matter distribution patterns (e.g. posterior in MLD, peritrigonal in Krabbe) |
| Progressive Multifocal Leukoencephalopathy (PML) | Ill-defined and diffusion restricting, unlikely to enhance |