Annular Tear
Summary
- Annular tear refers to a disruption of the annulus fibrosus of an intervertebral disc
- Typically occurs due to degenerative changes or acute trauma
- Imaging findings include high-intensity zones on MRI and contrast enhancement of the outer annulus
Pathophysiology
- Annulus fibrosus consists of concentric layers of collagen fibers
- Tears can be:
- Concentric: Separation between annular layers
- Radial: Extend from nucleus pulposus to outer annulus
- Transverse: Separate the annulus from the endplate
- Annular tears can lead to disc herniation and discogenic pain
Demographics
- Most common in adults aged 30-50 years
- Higher prevalence in:
- Males
- Individuals with physically demanding occupations
- Those with a history of trauma or repetitive stress
Diagnosis
- Clinical presentation:
- Low back pain, often with radicular symptoms
- Pain may worsen with certain movements or positions
- Physical examination:
- Limited range of motion
- Positive straight leg raise test (for lower lumbar tears)
- Diagnostic tests:
- MRI is the gold standard for diagnosis
- Discography may be used in select cases
Imaging
- MRI findings:
- High-intensity zone (HIZ) on T2-weighted images
- Focal hyperintensity in the posterior annulus on T2-weighted images
- Contrast enhancement of the outer annulus on post-gadolinium T1-weighted images
- CT discography:
- Contrast leakage into the annular tear
- Useful for correlating pain with specific disc levels
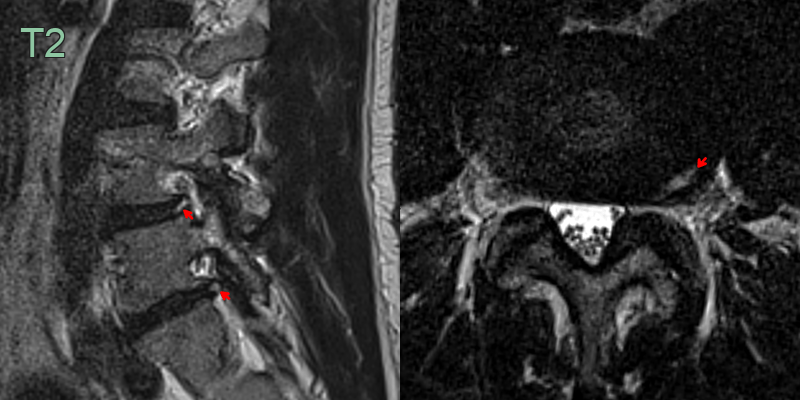
- A 45-year-old patient presented with an acute radiculopathy in the left L4 distribution.
- While there was only minimal intervertebral foraminal narrowing, the L4-5 disc that contained a T2-hyperintense annular tear made contact with the left L4 nerve root.
Treatment
- Conservative management:
- Physical therapy and exercise
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Activity modification
- Interventional procedures:
- Epidural steroid injections
- Intradiscal electrothermal therapy (IDET)
- Radiofrequency ablation
- Surgical options (for persistent symptoms):
- Microdiscectomy
- Disc replacement
- Spinal fusion (in select cases)
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Disc Herniation | Focal protrusion of disc material on MRI; may have associated nerve root compression |
| Facet Joint Arthropathy | Pain typically worse with extension; facet joint hypertrophy on imaging |
| Spinal Stenosis | Symptoms worsen with extension and improve with flexion; narrowing of spinal canal on imaging |
| Spondylolisthesis | Forward slippage of vertebra visible on X-ray or CT; may have associated instability |
| Myofascial Pain Syndrome | Presence of trigger points; no specific imaging findings |
| Sacroiliac Joint Dysfunction | Pain localized to SI joint area; may show inflammation on MRI |
| Vertebral Compression Fracture | Visible fracture on imaging; often associated with osteoporosis or trauma |
| Spinal Tumor | Mass lesion visible on MRI; may have associated systemic symptoms |
| Ankylosing Spondylitis | Fusion of sacroiliac joints on imaging; often affects younger males |
| Infection (Discitis/Osteomyelitis) | Fever, elevated inflammatory markers; visible infection on MRI with contrast |