Autosomal Recessive Spastic Ataxia of Charlevoix-Saguenay (ARSACS)¶
Summary

- ARSACS is a rare neurodegenerative disorder characterised by early-onset cerebellar ataxia, spasticity, and peripheral neuropathy
- Caused by mutations in the SACS gene, leading to progressive cerebellar and spinal cord degeneration
- Imaging reveals cerebellar atrophy, particularly of the superior vermis, and linear hypointensities in the pons on T2-weighted MRI
Pathophysiology¶
- Autosomal recessive inheritance pattern
- Mutations in the SACS gene on chromosome 13q12.12
- SACS gene encodes sacsin protein, involved in protein folding and quality control
- Loss of sacsin function leads to:
- Mitochondrial dysfunction
- Accumulation of neurofilaments
- Progressive neurodegeneration, particularly in the cerebellum and spinal cord
Demographics¶
- Originally described in the Charlevoix-Saguenay region of Quebec, Canada
- Prevalence in this region: 1 in 1,932 individuals
- Worldwide prevalence: rare, with cases reported in various populations
- Typical age of onset: early childhood (12-18 months)
- Equal gender distribution
Diagnosis¶
- Clinical presentation:
- Early-onset ataxia (unsteady gait)
- Progressive spasticity
- Peripheral neuropathy
- Dysarthria
- Nystagmus
- Genetic testing:
- Identification of biallelic pathogenic variants in the SACS gene
- Electromyography and nerve conduction studies:
- Evidence of axonal-demyelinating sensorimotor neuropathy
Imaging¶
- MRI findings:
- Cerebellar atrophy, particularly of the superior vermis
- Linear hypointensities in the pons on T2-weighted images ("Tiger stripe" appearance)
- Cervical spinal cord atrophy
- Cerebral cortical atrophy (in advanced cases)
- Spinal cord imaging:
- Thinning of the cervical and thoracic spinal cord
- Optical Coherence Tomography (OCT):
- Thickening of the retinal nerve fibre layer
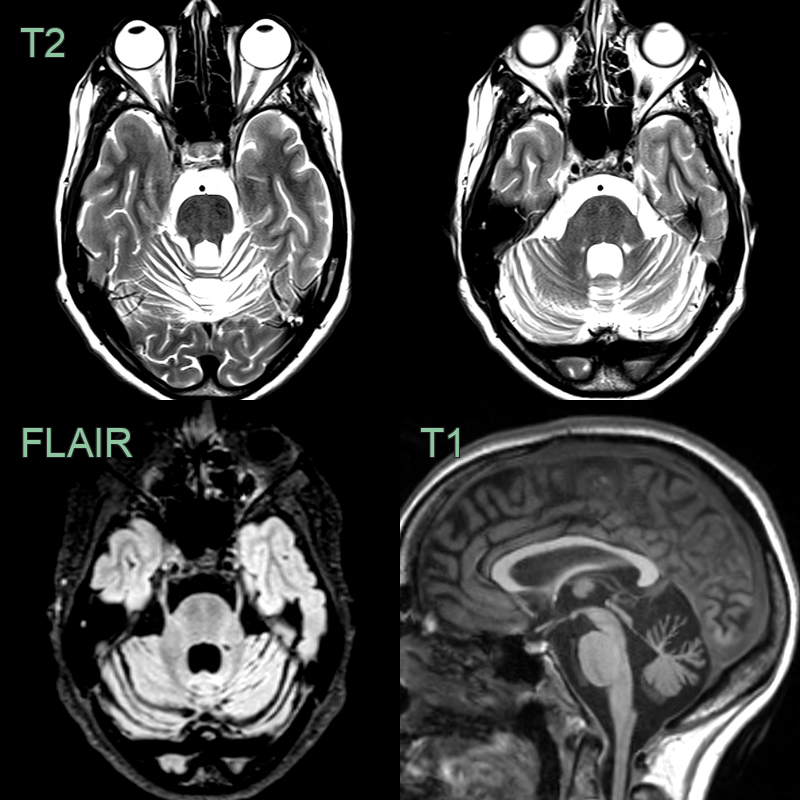
- Subtle symmetrical tigroid T2-hypointensity within the pons and severe superior cerebellar vermian atrophy.
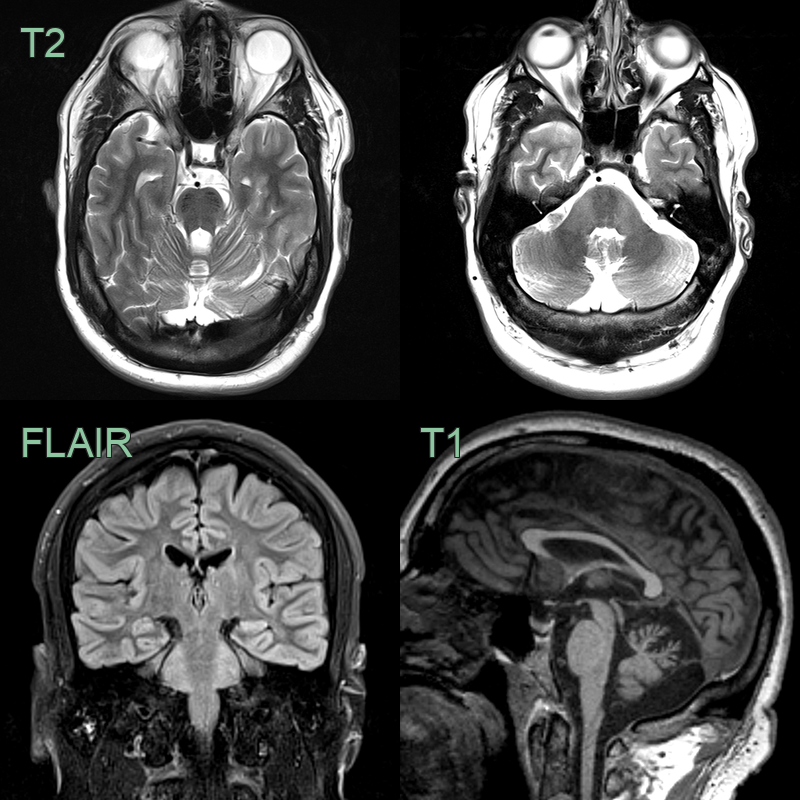
- 35-year-old patient presented with ataxia.
- MRI showed atrophy of the superior vermis, hyperintensity in the middle cerebellar peduncles and, most characteristically, tigroid T2-hypointensity within the pons.
Treatment¶
- No curative treatment available
- Management focuses on symptomatic relief and supportive care:
- Physical therapy to maintain mobility and prevent contractures
- Occupational therapy for activities of daily living
- Speech therapy for dysarthria
- Anti-spasticity medications (e.g., baclofen) for spasticity
- Ankle-foot orthoses for gait stability
- Regular monitoring of cardiac function
- Genetic counseling for affected individuals and families
- Ongoing research into potential gene therapy approaches
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Friedreich's Ataxia | Absence of hypermyelination of retinal nerve fibres; cardiomyopathy is common |
| Hereditary Spastic Paraplegia | Usually lacks cerebellar ataxia; no retinal changes |
| Ataxia-Telangiectasia | Presence of telangiectasias; immunodeficiency; elevated alpha-fetoprotein |
| Charcot-Marie-Tooth Disease | Predominantly peripheral neuropathy; lacks spasticity |
| Multiple Sclerosis | Relapsing-remitting course; white matter lesions on MRI |
| Spinocerebellar Ataxia | Later onset; often autosomal dominant inheritance |
| Cerebellar Ataxia with Neuropathy and Vestibular Areflexia Syndrome (CANVAS) | Presence of vestibular areflexia; absence of spasticity |
| Ataxia with Vitamin E Deficiency | Low serum vitamin E levels; improvement with vitamin E supplementation |
| Refsum Disease | Presence of anosmia; ichthyosis; retinitis pigmentosa |
| Cerebrotendinous Xanthomatosis | Presence of tendon xanthomas; cataracts; cognitive decline |