Arteriovenous Malformation¶
Summary
- Congenital vascular anomaly characterised by abnormal connections between arteries and veins, bypassing the capillary bed
- Most commonly occurs in the brain, but can affect any organ system
- Presents with haemorrhage, seizures, or neurological deficits in cerebral AVMs
Pathophysiology¶
- Abnormal development of embryonic vascular system
- Direct arteriovenous shunting without intervening capillary network
- Progressive dilation of feeding arteries and draining veins
- Risk of rupture due to high-flow, high-pressure system
Demographics¶
- Prevalence: 18 per 100,000 adults
- Male to female ratio: 1:1
- Most common age of presentation: 20-40 years
- Sporadic occurrence in majority of cases
- Associated with hereditary haemorrhagic telangiectasia in some cases
Diagnosis¶
- Clinical presentation:
- Intracranial haemorrhage (50%)
- Seizures (30%)
- Headaches (15%)
- Focal neurological deficits (5%)
- Physical examination:
- May be normal
- Focal neurological deficits
- Bruit on auscultation (rare)
- Laboratory tests:
- Generally not specific for AVM diagnosis
Imaging¶
- Computed Tomography (CT):
- Non-contrast CT: Hyperdense serpiginous structures
- CT Angiography: Delineates feeding arteries and draining veins
- Magnetic Resonance Imaging (MRI):
- T1-weighted: Flow voids
- T2-weighted: Mixed signal intensity
- Susceptibility-weighted imaging: Haemosiderin deposition from previous haemorrhage
- Digital Subtraction Angiography (DSA):
- Gold standard for diagnosis and treatment planning
- Demonstrates nidus, feeding arteries, and draining veins
- Allows assessment of flow dynamics
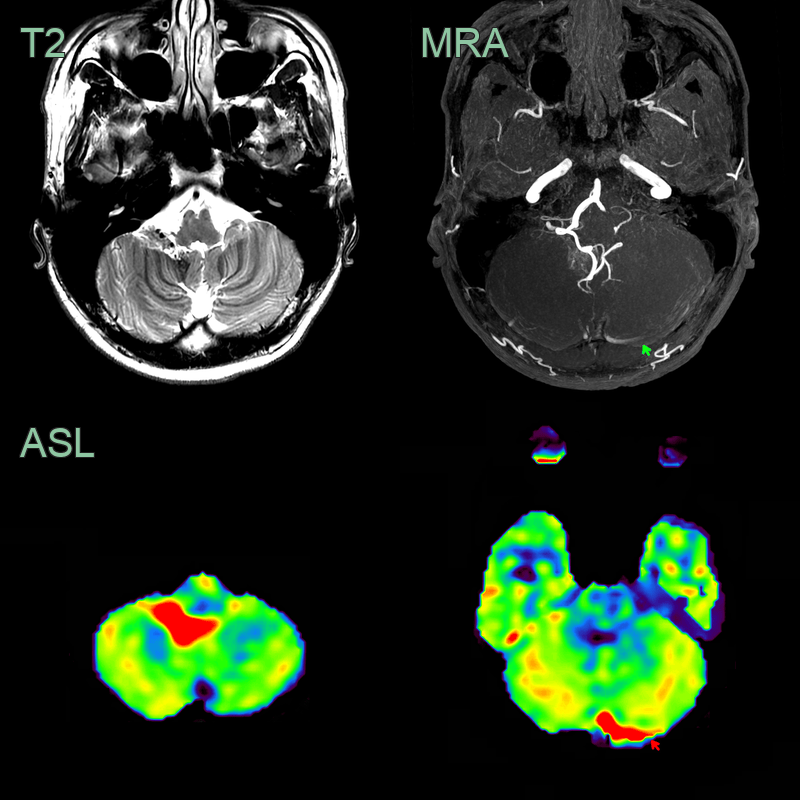
- A 30-year-old patient presented with right sided pulsatile tinnitus.
- Time-of-flight angiography showed a hypertrophied right PICA and a small AVM nidus near the fourth ventricle.
- Confirmed with ASL, the lesion was associated with shunting into the left transverse sinus (high signal on ToF MRA and elevated CBF on ASL).
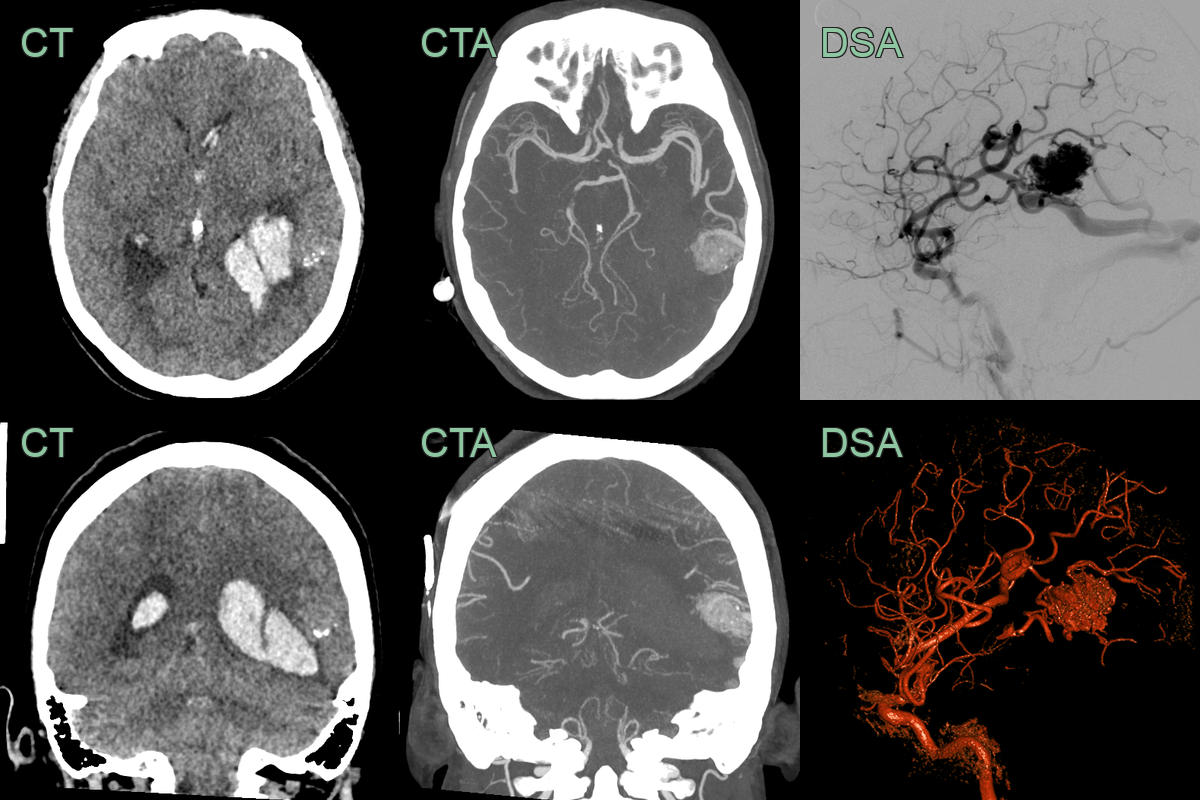
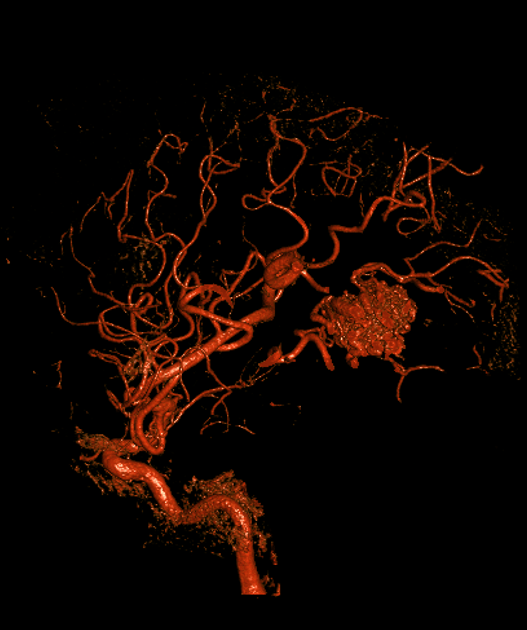
- A 40-year-old patient presented with a headache and right sided weakness.
- CT showed a left temporal haematoma with associated calcification.
- CTA and DSA showed an arteriovenous malformation supplied by the left MCA with cortical drainage.
Treatment¶
- Conservative management:
- Observation for small, asymptomatic AVMs
- Medical management of symptoms (e.g., anticonvulsants for seizures)
- Microsurgical resection:
- Complete removal of AVM
- Preferred for superficial, accessible lesions
- Endovascular embolisation:
- Occlusion of feeding arteries using embolic agents
- Can be used as adjunct to surgery or radiosurgery
- Stereotactic radiosurgery:
- Focused radiation to induce gradual AVM obliteration
- Suitable for small, deep-seated AVMs
- Multimodality treatment:
- Combination of above techniques for complex AVMs
- Follow-up imaging:
- DSA or MRI to assess treatment efficacy and recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cavernous malformation | Lack of arterial flow on angiography |
| Capillary telangiectasia | Smaller size and less prominent on imaging |
| Developmental venous anomaly | Characteristic "caput medusae" appearance on contrast-enhanced imaging |
| Tumour (e.g., glioma) | Presence of mass effect and surrounding oedema |
| Cerebral aneurysm | Typically appears as a saccular outpouching on a vessel |
| Moyamoya disease | Bilateral involvement of internal carotid arteries with characteristic "puff of smoke" appearance |
| Dural arteriovenous fistula | Direct connection between dural arteries and venous sinuses |
| Sturge-Weber syndrome | Associated facial port-wine stain and leptomeningeal angiomatosis |
| Cerebral abscess | Ring-enhancing lesion with surrounding oedema and fever |
| Multiple sclerosis | Ovoid periventricular white matter lesions on MRI |