Artery of Percheron infarct¶
Summary
- Infarct affecting the bilateral paramedian thalami and midbrain
- Caused by an occlusion of the artery of Percheron, a single, azygos, arterial trunk supplying both thalami
- May present with altered mental status/GCS, vertical gaze palsy, and memory impairment
Pathophysiology¶
- Artery of Percheron: anatomical variant of posterior cerebral circulation
- Single, azygos, arterial trunk arising from P1 segment of one posterior cerebral artery
- Supplies bilateral paramedian thalami and midbrain
- Occlusion leads to:
- Bilateral thalamic infarction
- Possible midbrain involvement
Diagnosis¶
- Clinical presentation:
- Altered mental status (ranging from confusion to coma)
- Vertical gaze palsy
- Memory impairment
- Possible oculomotor disturbances
- Differential diagnosis:
- Top of the basilar syndrome
- Wernicke encephalopathy
- Viral encephalitis
- Deep cerebral venous thrombosis
Imaging¶
- CT:
- Early: may be normal or show subtle hypodensity in bilateral thalami
- Late: bilateral paramedian thalamic hypodensities ± midbrain involvement
- May see hyperdense thrombus within PCA. Hyperdense thrombus within the Artery of Percheron is unlikely to be seen as it is so small
- MRI:
- DWI/ADC: early detection of acute infarction
- T2/FLAIR: hyperintense signal in affected areas after ~4 hours
- Characteristic "V-sign" on axial images (paramedian thalamic involvement)
- CT/MR angiography:
- May show occlusion or absence of artery of Percheron
- Often challenging due to small vessel size
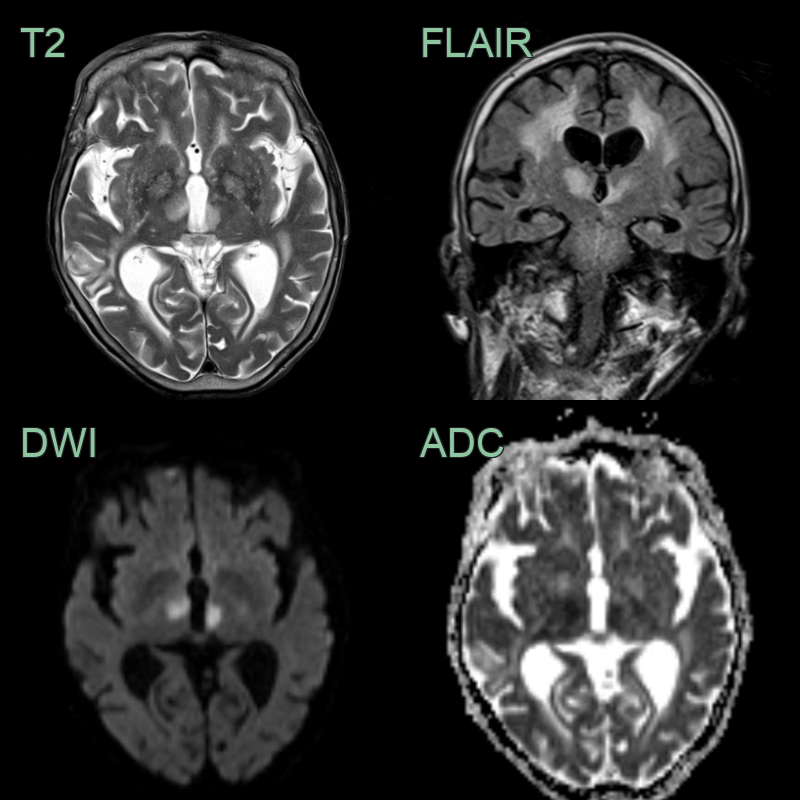
- A 70-year-old patient presented with confusion and vertical gaze palsy.
- Acute bithalamic infarcts are in the territory of the artery of Percheron.
Treatment¶
- Acute management:
- Thrombolysis if within time window and no contraindications
- Mechanical thrombectomy in select cases where thrombus is present in larger artery (PCA or basilar artery)
- Secondary prevention:
- Antiplatelet therapy or anticoagulation based on etiology
- Risk factor modification (hypertension, diabetes, hyperlipidaemia)
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Top of the basilar syndrome | Additional involvement of midbrain, occipital lobes, or cerebellum |
| Wernicke encephalopathy | Mammillary body and periaqueductal grey T2 hyperintensity; thalamic involvement more variable |
| Viral encephalitis (e.g. EBV, flavivirus) | Thalamic T2 hyperintensity with lobar involvement; leptomeningeal enhancement |
| Midline glioma | Mass effect; contrast enhancement; slower onset |
| Carbon monoxide poisoning | History of exposure; globus pallidus involvement |
| MELAS | Non-vascular-territory cortical/subcortical DWI restriction; lactate peak on MRS |
| Creutzfeldt-Jakob disease | Cortical ribboning on DWI; rapidly progressive dementia |