Aseptic Meningitis¶
Summary
- Inflammation of the meninges without bacterial infection
- Typically caused by viruses, but can also be due to drugs, autoimmune conditions, or malignancies
- Characterised by fever, headache, and neck stiffness with negative bacterial cultures
Pathophysiology¶
- Viral invasion of the central nervous system (CNS)
- Direct infection of meningeal and ependymal cells
- Immune-mediated inflammation
- Non-viral causes:
- Drug-induced hypersensitivity reactions
- Autoimmune processes (e.g., systemic lupus erythematosus)
- Paraneoplastic syndromes
Demographics¶
- Can affect all age groups
- More common in children and young adults
- Seasonal variation:
- Enteroviruses peak in summer and early fall
- Arboviruses more prevalent in warmer months
Diagnosis¶
- Clinical presentation:
- Fever, headache, neck stiffness
- Photophobia, nausea, vomiting
- Cerebrospinal fluid (CSF) analysis:
- Pleocytosis (>5 white blood cells/μL)
- Normal or mildly elevated protein
- Normal glucose
- Negative bacterial cultures
- Polymerase chain reaction (PCR) for viral pathogens
- Serology for specific viral antibodies
Imaging¶
- Neuroimaging not routinely required for uncomplicated cases
- MRI findings (when performed):
- Normal in most cases
- Possible leptomeningeal enhancement
- Exclude complications or alternative diagnoses
- CT scan:
- Limited role in diagnosis
- May be used to rule out increased intracranial pressure before lumbar puncture
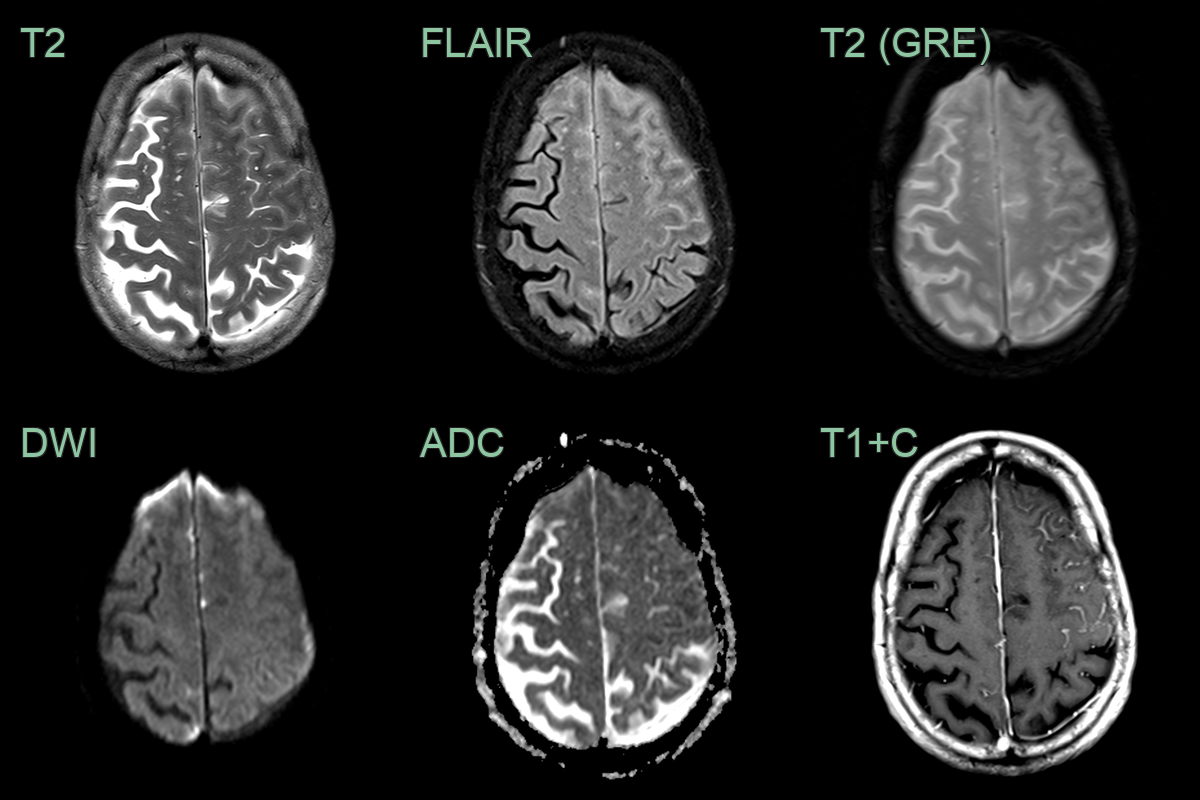
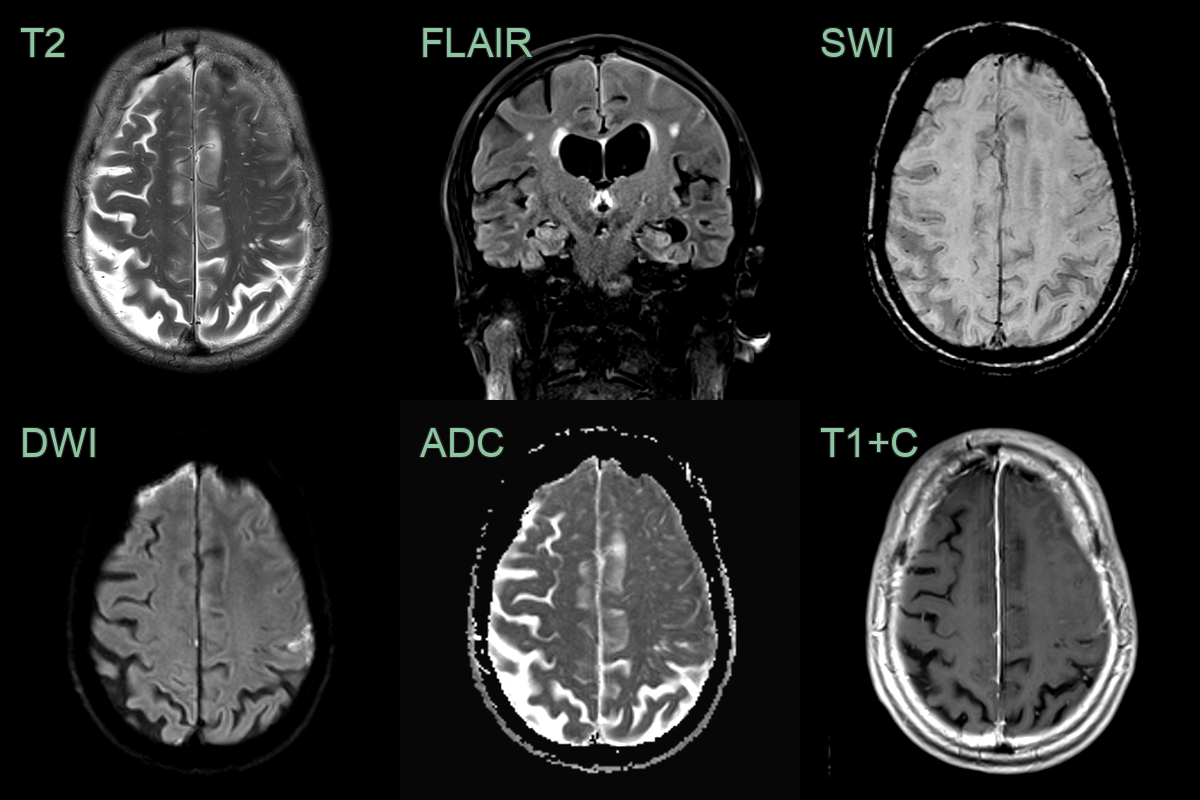
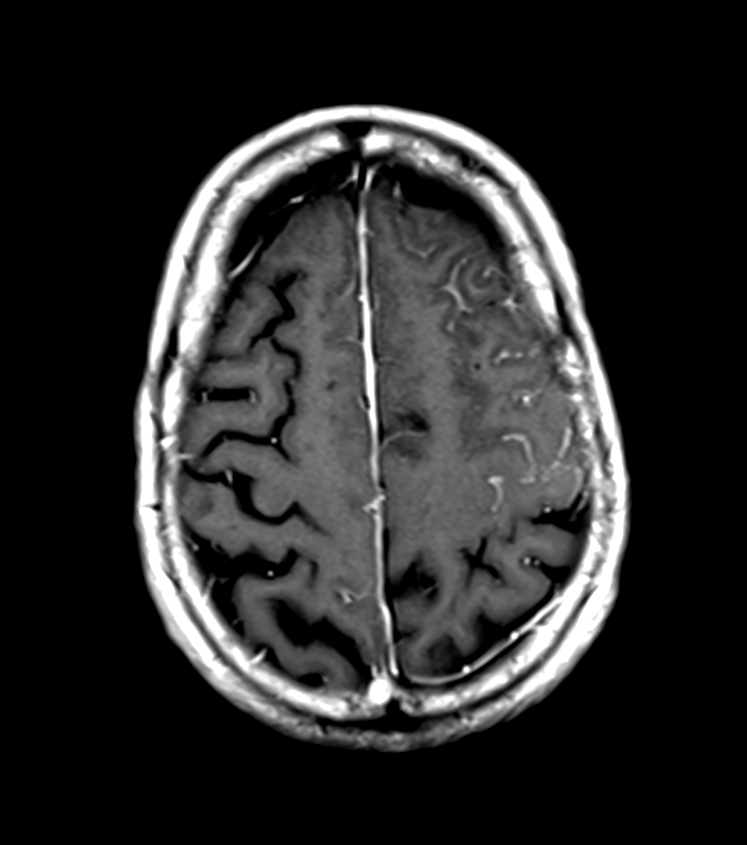
- A 70-year-old patient presented with dysarthria and and right sided upper limb numbness.
- FLAIR and diffusion-weighted sulcal hyperintensity and leptomeningeal enhancement regressed after two months of a tapering steroid regimen.
- Biopsy revealed a chronic lymphocystic meningitis that was assumed to be related to the patient's longstanding rheumatoid arthritis.
Treatment¶
- Supportive care:
- Hydration
- Analgesics for pain and fever
- Anti-emetics for nausea
- Antiviral therapy:
- Acyclovir for suspected herpes simplex virus (HSV) meningitis
- Ganciclovir for cytomegalovirus (CMV) meningitis
- Discontinuation of offending drugs in drug-induced cases
- Immunomodulatory therapy for autoimmune causes
- Monitoring for potential complications:
- Increased intracranial pressure
- Seizures
- Cognitive impairment
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Bacterial Meningitis | Diffuse intense leptomeningeal enhancement; may show cerebritis, subdural empyema, or hydrocephalus on MRI |
| Viral Encephalitis | Temporal lobe and limbic T2/FLAIR signal abnormality on MRI; cortical restricted diffusion in active disease |
| Tuberculous Meningitis | Basilar predominant meningeal enhancement; perforator territory infarcts; communicating hydrocephalus |
| Subarachnoid Haemorrhage | Hyperdense cisternal blood on CT; sulcal FLAIR signal without enhancement pattern |
| Brain Abscess | Ring-enhancing lesion with restricted DWI centrally; smooth thin capsule; surrounding vasogenic oedema |
| Neoplastic Meningitis | Nodular leptomeningeal enhancement along cranial nerves, spinal roots and pia; may show communicating hydrocephalus |
| Autoimmune Meningitis | Smooth or nodular pachymeningeal or leptomeningeal enhancement; hypothalamic or infundibular involvement in some subtypes |