Astrocytoma¶
Summary
- Astrocytomas are primary brain tumours arising from astrocytes, characterised by infiltrative growth patterns
- Clinical presentation varies based on tumour location and grade, ranging from seizures to focal neurological deficits
- Imaging features include variable enhancement, oedema, and mass effect, with higher-grade tumours showing more aggressive characteristics
Pathophysiology¶
- Originate from astrocytes, star-shaped glial cells that support neuronal function
- Classified by WHO into four grades (I-IV) based on histological features and molecular markers
- Key genetic alterations include:
- IDH½ mutations (common in lower-grade astrocytomas)
- TP53 mutations
- ATRX mutations
- EGFR amplification (in glioblastoma, WHO grade 4)
Demographics¶
- Incidence: 5-6 per 100,000 person-years
- Age distribution:
- Low-grade astrocytomas: peak incidence in young adults (20-40 years)
- High-grade astrocytomas: more common in older adults (>50 years)
- Slight male predominance (M:F ratio 1.2:1)
- Risk factors:
- Exposure to high-dose ionising radiation
- Certain genetic syndromes (e.g., neurofibromatosis type 1, Li-Fraumeni syndrome)
Diagnosis¶
- Clinical presentation:
- Seizures (most common initial symptom in low-grade astrocytomas)
- Headaches
- Focal neurological deficits
- Cognitive changes
- Diagnostic workup:
- Neuroimaging (MRI with and without contrast)
- Stereotactic biopsy or surgical resection for histopathological diagnosis
- Molecular testing for IDH mutation, 1p/19q codeletion, and MGMT promoter methylation status
Imaging¶
- MRI is the imaging modality of choice
- Low-grade astrocytomas (WHO grade 2):
- T1: hypointense
- T2/FLAIR: hyperintense
- Minimal or no enhancement
- Little or no perilesional oedema
- High-grade astrocytomas (WHO grade 3–4):
- T1: hypointense with heterogeneous signal
- T2/FLAIR: hyperintense with surrounding oedema
- Variable enhancement patterns (ring-enhancing in glioblastoma)
- Mass effect and midline shift in larger tumours
- Advanced imaging techniques:
- Perfusion imaging: increased relative cerebral blood volume (rCBV) in higher-grade tumours
- MR spectroscopy: elevated choline peak, reduced N-acetylaspartate (NAA)
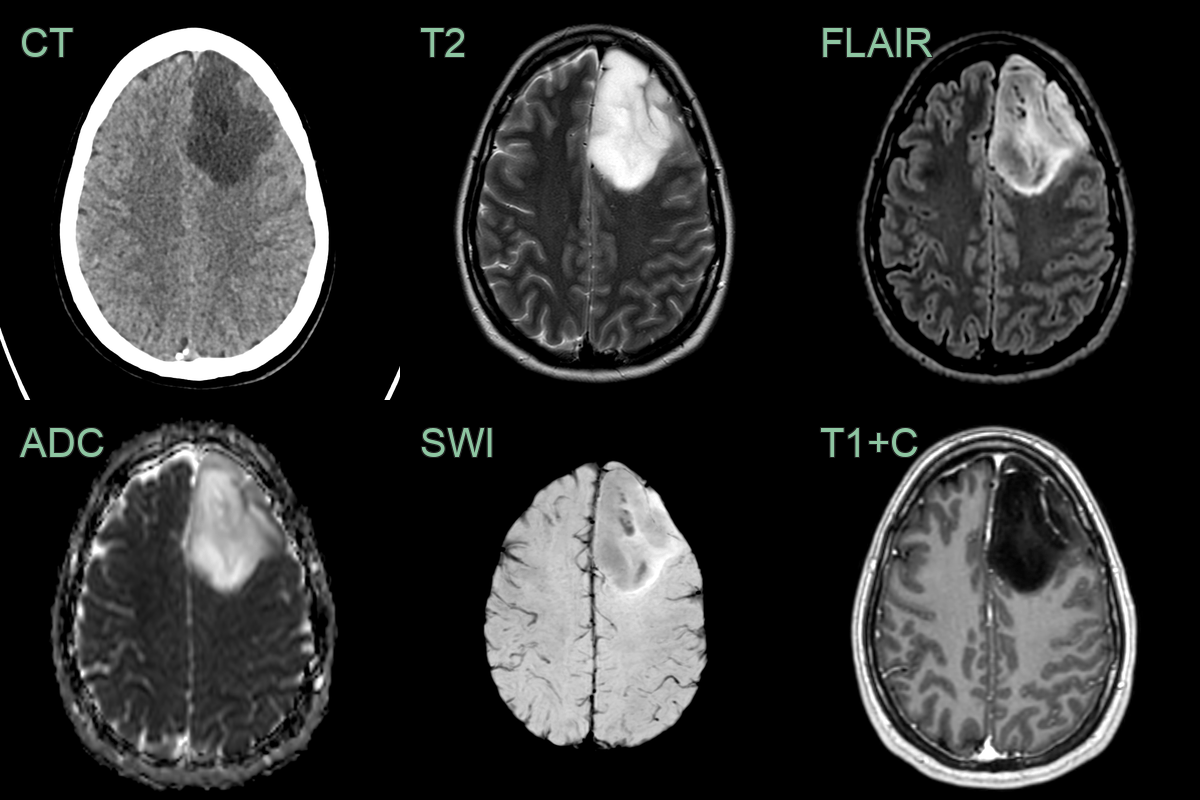
- 35-year-old patient with 2 month history of headache presented after a tonic-clonic seizure.
- Imaging showed a quite well defined T2-hyperintense non-enhancing lesion.
- Low FLAIR signal in more than half of the tumour representing the T2-FLAIR mismatch sign suggested an astrocytoma that was confirmed on histopathology following resection.
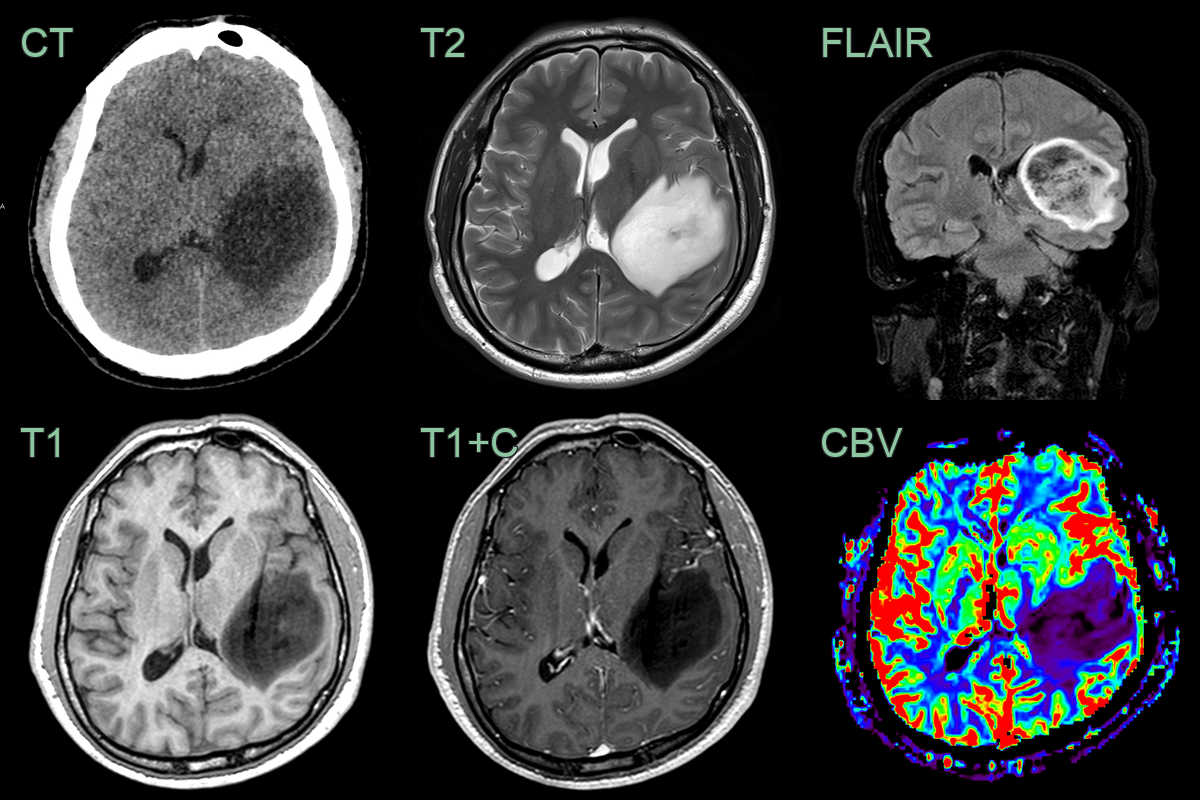
- A 35-year-old patient presented with a worsening headache and blurry vision.
- Imaging showed a large subcortical lesion centred in the left temporal lobe.
- The low CBV and T2-FLAIR mismatch sign were compatible with the histopathological diagnosis of a grade 2 astrocytoma.
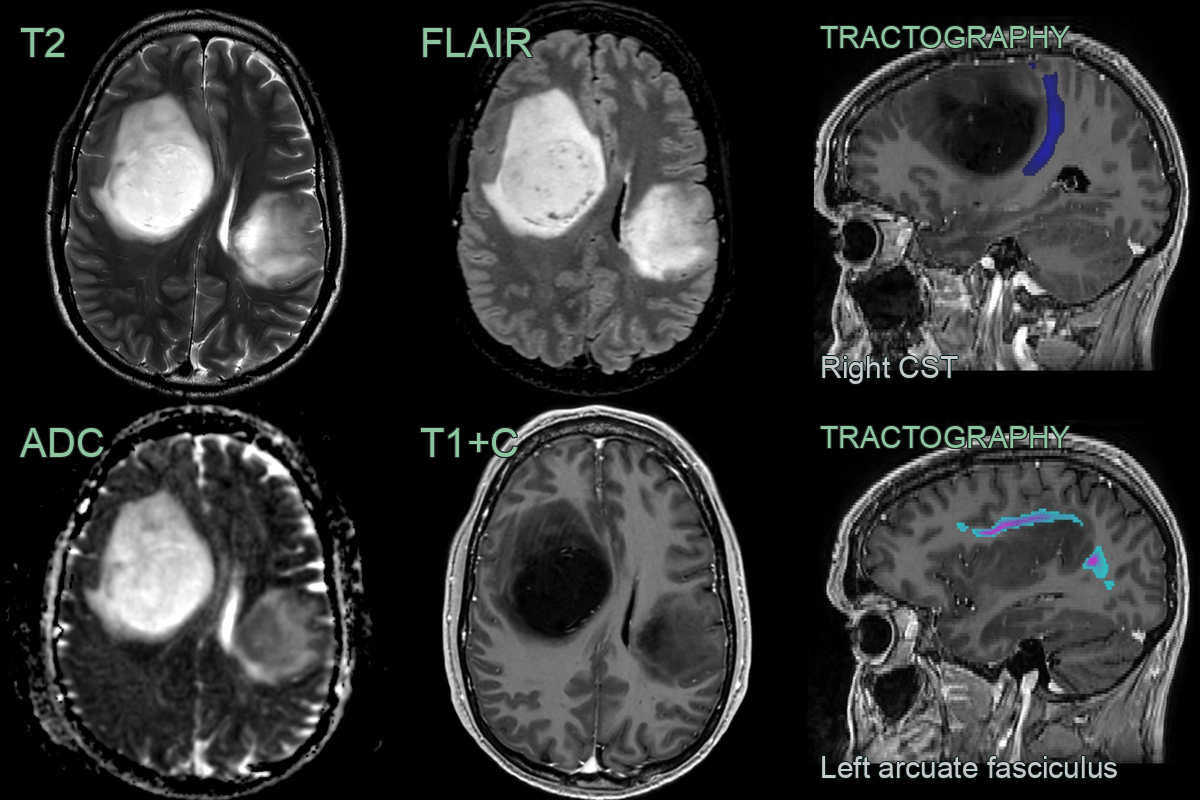
- A 40 year old presented with with memory issues and headache.
- MRI showed two large lesions, one in each hemisphere that did not show any enhancement but there were low ADC values within the left sided lesion.
- Initial histopathlogy suggested a grade 2 astrocytoma however, following molecular anlysis, this was upgrade to a grade 4 astrocytoma on the basis of a CDKN2A/B deletion.
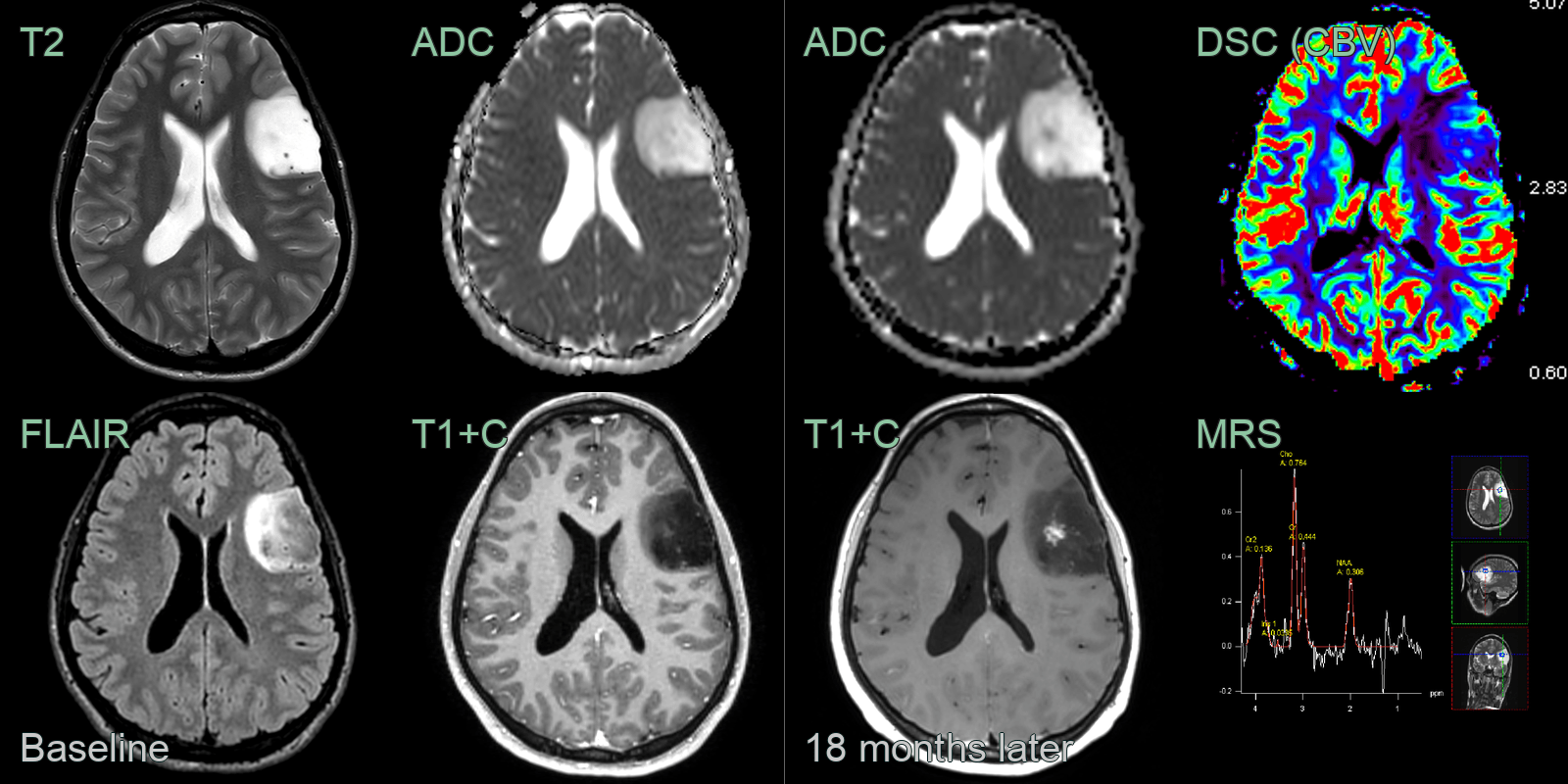
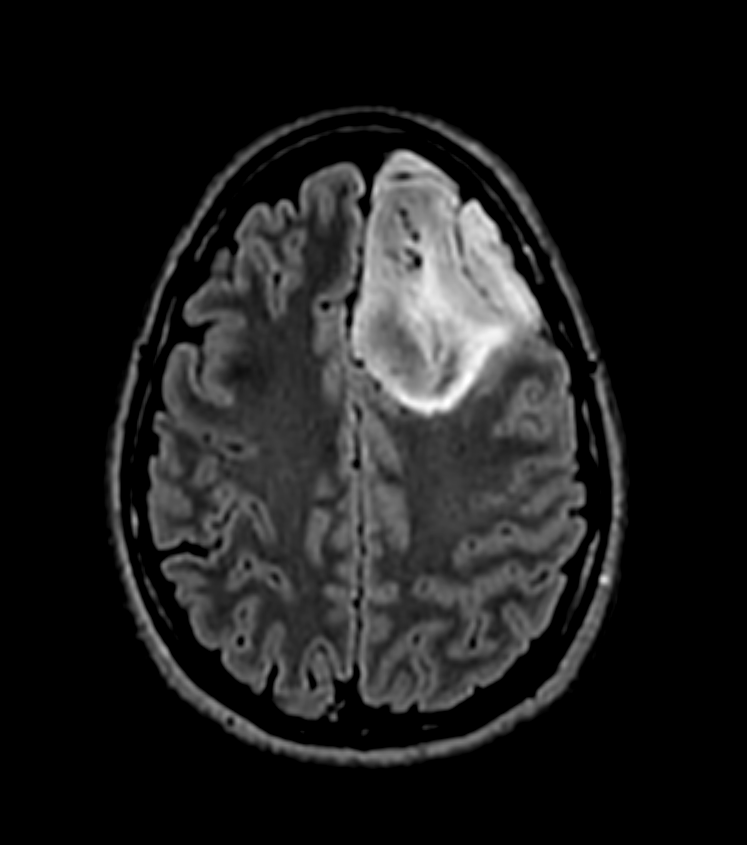
- A 20-year-old patient with Li Fraumeni Syndrome presented following a seizure.
- MRI showed a left frontal lesion with a T2-FLAIR mismatch (hyperintense on T2 and more than half of the lesion hypointense on FLAIR).
- On follow-up imaging 18 months later, spiculated enhancement developed iwthin the tumour, which corresponded to an a region of low values on ADC.
- CBV was elevated (ratio of 4 relative to normal appearing brain tissue) and MR spectrscopy showed reversal of Hunter's angle (elevated choline and reduced NAA).
- Following resection, a grade 3 astrocytoma was diagnosed.
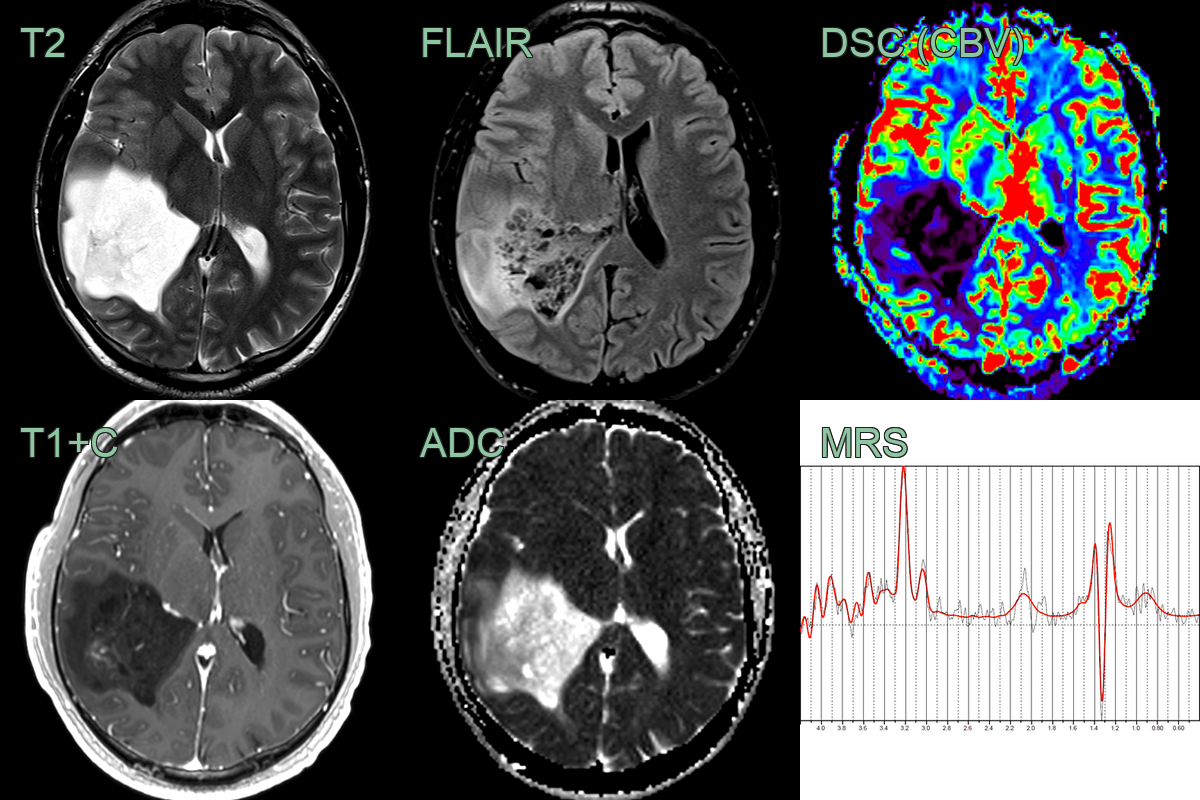
- A 30-year-old patient presented following a seizure.
- MRI showed a large right parietal lesion with a T2-FLAIR mismatch.
- A region of enhancement corresponded to a region of relative hypercelluarity and higher CBV.
- MRS was very abnormal with grossly reduced NAA, elevated choline, and the presence of lactate.
- Final molecular diagnosis was a grade 4 astrocytoma.
Treatment¶
- Management approach depends on tumour grade, location, and patient factors
- Low-grade astrocytomas:
- Observation with serial imaging for asymptomatic patients
- Maximal safe surgical resection when feasible
- Adjuvant radiotherapy and/or chemotherapy for high-risk patients
- High-grade astrocytomas:
- Maximal safe surgical resection
- Adjuvant radiotherapy with concurrent and adjuvant temozolomide (Stupp protocol)
- Consider tumour-treating fields (TTFields) for glioblastoma
- Supportive care:
- Anti-epileptic drugs for seizure control
- Corticosteroids for perilesional oedema
- Rehabilitation and psychosocial support
- Emerging therapies:
- Targeted molecular therapies (e.g., IDH inhibitors)
- Immunotherapy approaches (e.g., checkpoint inhibitors, CAR-T cell therapy)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Oligodendroglioma | Calcifications on CT, "chicken wire" vasculature |
| Metastasis | Multiple lesions; ring or nodular enhancement; grey-white junction predilection; surrounding vasogenic oedema disproportionate to lesion size |
| Lymphoma | More homogeneous enhancement; periventricular location; restricted diffusion on DWI; hyperdense on non-contrast CT |
| Ependymoma | Intraventricular location; calcifications; ependymal spread |
| Glioblastoma | Central necrosis with ring enhancement; marked surrounding oedema; crosses corpus callosum |
| Pilocytic astrocytoma | Cystic component with enhancing mural nodule; well-defined margins; posterior fossa predilection in children |
| Demyelinating disease | Incomplete ring enhancement open towards cortex; perivenular distribution on sagittal FLAIR; multiple lesions |
| Abscess | Restricted diffusion on DWI with low ADC; smooth thin ring enhancement; may have satellite lesions |
| Meningioma | Extra-axial location, dural tail sign |
| Ganglioglioma | Calcifications, cystic component, temporal lobe predilection |