Autoimmune Encephalitis¶
Summary
- Autoimmune encephalitis encompasses a group of inflammatory brain disorders caused by antibodies targeting neuronal cell surface or synaptic proteins
- Presents with subacute onset of memory deficits, altered mental status, psychiatric symptoms, and seizures
- MRI typically shows T2/FLAIR hyperintensity in medial temporal lobes, though can be normal in up to 50% of cases
Pathophysiology¶
- Antibody-mediated mechanisms
- Cell surface/synaptic protein antibodies (e.g., NMDAR, LGI1, CASPR2, AMPAR, GABA-B receptor)
- Intracellular antibodies (e.g., anti-Hu, anti-Ma2, anti-GAD65)
- Pathogenic processes
- Receptor internalization and decreased synaptic density
- Direct blockade of receptor function
- Complement activation and neuronal damage
- Associated triggers
- Paraneoplastic (ovarian teratoma with anti-NMDAR, small cell lung cancer with anti-Hu)
- Post-infectious (HSV encephalitis preceding anti-NMDAR encephalitis)
- Idiopathic
Demographics¶
- Age distribution
- Anti-NMDAR: predominantly young adults and children (median age 20-25 years)
- Anti-LGI1: older adults (median age 60-65 years)
- Anti-CASPR2: middle-aged to older men
- Gender predilection
- Anti-NMDAR: female predominance (4:1), especially with ovarian teratoma
- Anti-LGI1 and CASPR2: male predominance (2:1)
- Incidence
- Estimated 0.8-1.2 per 100,000 person-years
- Anti-NMDAR is most common, accounting for ~80% of cases
Diagnosis¶
- Clinical presentation
- Prodromal phase: headache, fever, flu-like symptoms
- Psychiatric symptoms: psychosis, agitation, catatonia, hallucinations
- Memory deficits and cognitive dysfunction
- Seizures (focal or generalized)
- Movement disorders: orofacial dyskinesias, choreoathetosis, dystonia
- Autonomic dysfunction: cardiac arrhythmias, hyperthermia, hypoventilation
- Laboratory findings
- CSF: lymphocytic pleocytosis, elevated protein, oligoclonal bands
- Antibody testing: serum and CSF (CSF more sensitive)
- EEG: extreme delta brush pattern (anti-NMDAR), focal temporal abnormalities
- Diagnostic criteria
- Probable: compatible clinical syndrome with CSF pleocytosis or EEG/MRI abnormalities
- Definite: antibody positive with compatible clinical syndrome
Imaging¶
- MRI findings
- T2/FLAIR: hyperintense signal in medial temporal lobes (hippocampi, amygdala)
- T2/FLAIR: cortical/subcortical hyperintensities in other regions (frontal, parietal, insular)
- T2/FLAIR: basal ganglia hyperintensity (particularly in anti-NMDAR)
- T1: typically isointense to hypointense in affected regions
- T1+C: variable enhancement (mild leptomeningeal or parenchymal)
- DWI: restricted diffusion uncommon, may occur in severe cases
- SWI: usually normal, occasional microhaemorrhages in severe cases
- Pattern by antibody type
- Anti-NMDAR: normal MRI in 50-60%, or T2 hyperintensity in hippocampi, cortex, subcortical regions
- Anti-LGI1: unilateral or bilateral medial temporal T2/FLAIR hyperintensity
- Anti-CASPR2: medial temporal and basal ganglia T2 hyperintensity
- Anti-GABA-B: bilateral medial temporal T2 hyperintensity with restricted diffusion
- **FDG-PET findings
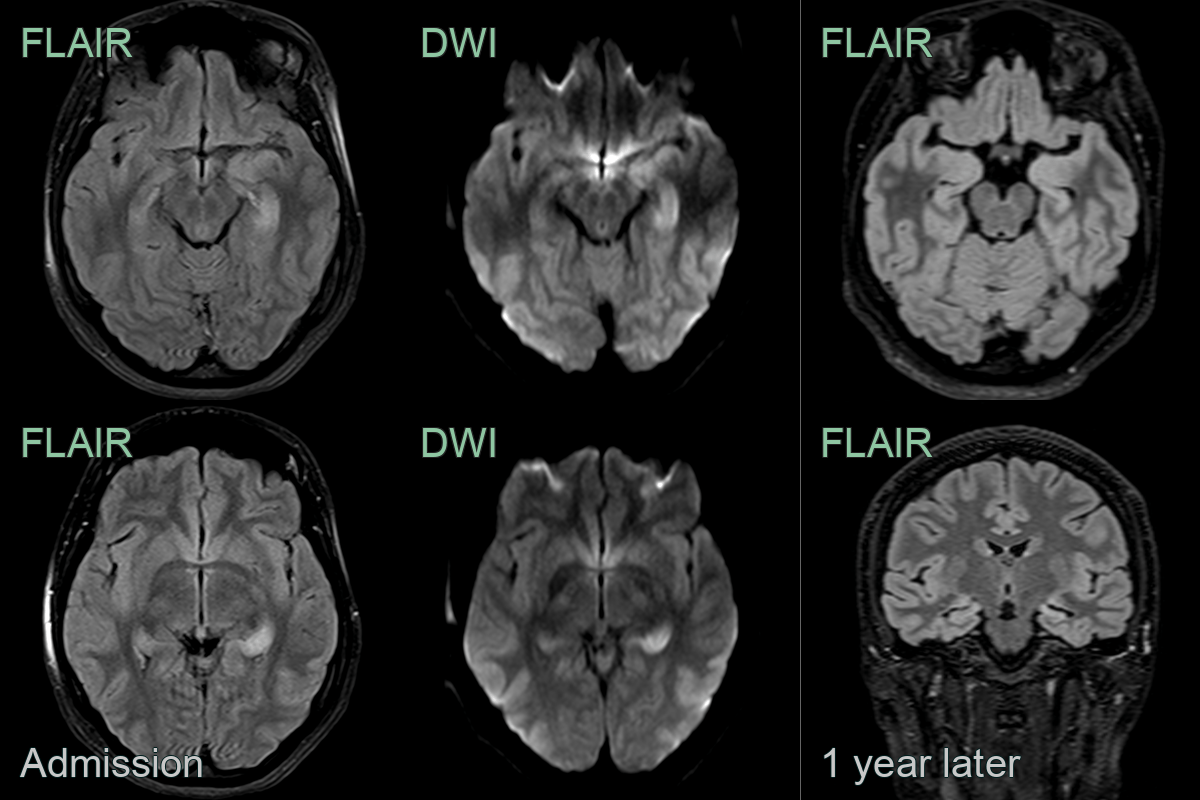
- A 20-year-old patient presented with confusion, headache and low grade fever.
- MRI showed swelling and FLAIR and DWI hyperintensity affecting the hippocampi (L>>R).
- GABA-B antibodies were identified within CSF.
- 1 year later, the hyperintensity persisted within atrophic hippocampi.
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Viral encephalitis (HSV) | Asymmetric medial temporal/insular FLAIR and DWI hyperintensity with haemorrhagic change |
| Primary CNS lymphoma | MRI shows enhancing mass lesions; CSF cytology/flow cytometry positive for malignant cells |
| Creutzfeldt-Jakob disease | Cortical ribbon and basal ganglia DWI restriction; pulvinar/hockey-stick sign |
| CNS vasculitis | Vessel wall enhancement on MRI; infarcts; microhaemorrhages, angiography shows beading/stenosis of vessels |
| Glioma (temporal lobe) | Mass effect; irregular enhancement; does not resolve on follow-up |
| Mitochondrial encephalopathy (MELAS) | Stroke-like cortical lesions not respecting vascular territories; lactate peak on MRS |