Basilar Artery Fenestration¶
Summary
- Basilar artery fenestration is a rare vascular anomaly characterised by the splitting of the basilar artery into two separate channels that later reunite
- Associated with increased risk of aneurysm formation and subarachnoid haemorrhage
- Typically asymptomatic and discovered incidentally on imaging studies
Pathophysiology¶
- Results from incomplete fusion of paired longitudinal neural arteries during embryonic development
- Fenestration can occur at any point along the basilar artery, but most commonly in the proximal segment
- Associated with weakened vessel walls and altered haemodynamics, potentially leading to aneurysm formation
Demographics¶
- Prevalence estimated at 0.6-2.3% in angiographic studies
- No significant gender predilection
- Can occur at any age, but typically discovered in adulthood during imaging for unrelated conditions
Diagnosis¶
- Usually asymptomatic and found incidentally
- May present with symptoms related to associated aneurysms or subarachnoid haemorrhage
- Rarely associated with ischaemic events due to thrombus formation within the fenestration
Imaging¶
- Digital Subtraction Angiography (DSA):
- Gold standard for diagnosis
- Demonstrates two separate lumens with reunification
- CT Angiography (CTA):
- High-resolution imaging can detect fenestrations
- May be limited by bone artefacts at the skull base
- MR Angiography (MRA):
- Time-of-flight (TOF) and contrast-enhanced techniques can visualise fenestrations
- Less sensitive than CTA or DSA for small fenestrations
- 3D rotational angiography:
- Provides detailed visualization of vascular anatomy
- Useful for surgical or endovascular planning
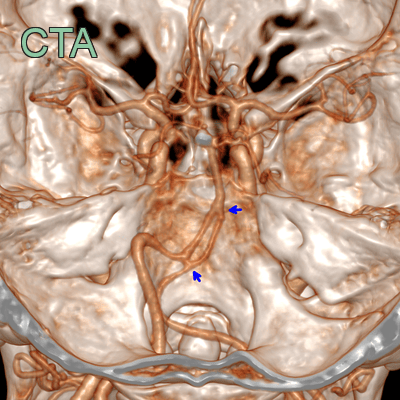
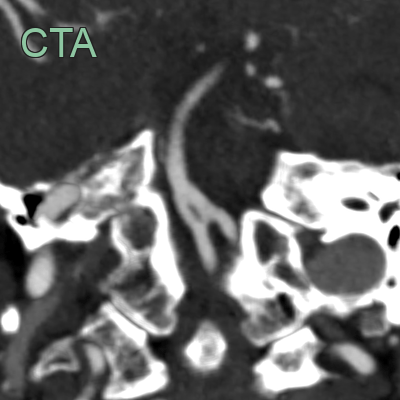
- After the confluence of the vertebral arteries, the the basilar artery diverges before merging at its mid-segment.
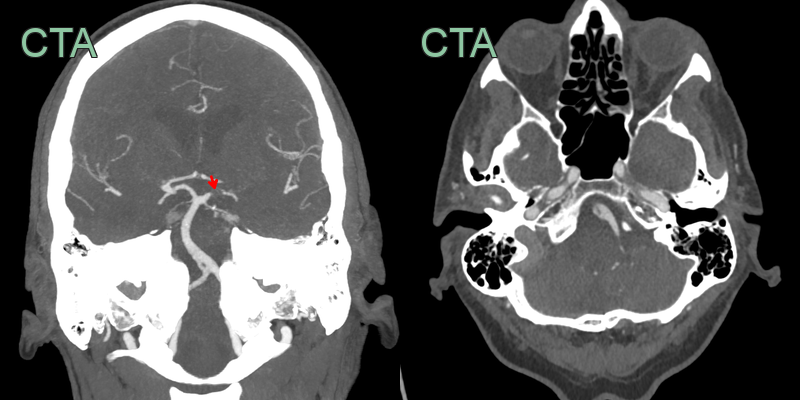
- Left PCA thrombus (red arrow) caused a left occipital infarct.
- There was a proximal basilar artery fenestration.
Treatment¶
- Asymptomatic fenestrations without associated aneurysms:
- No specific treatment required
- Regular imaging follow-up may be considered
- Associated aneurysms:
- Treatment options include surgical clipping or endovascular coiling
- Decision based on aneurysm size, location, and patient factors
- Endovascular considerations:
- Fenestrations may complicate endovascular procedures
- Careful planning and technique required to avoid compromising flow in either channel
- Thromboembolic events:
- Antiplatelet or anticoagulation therapy may be considered in cases of recurrent ischaemia
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Basilar artery dissection | Absence of intimal flap or double lumen on imaging |
| Vertebrobasilar dolichoectasia | Elongation and dilatation of basilar artery without focal splitting |
| Basilar artery aneurysm | Focal outpouching rather than longitudinal splitting of the artery |
| Arteriovenous malformation | Absence of abnormal arteriovenous connections on angiography |
| Basilar artery thrombosis | Lack of filling defect or occlusion on vascular imaging |
| Persistent trigeminal artery | Different anatomical location and connection to carotid artery |
| Basilar artery hypoplasia | Uniformly small caliber without focal duplication |
| Basilar artery atherosclerosis | Absence of focal arterial wall thickening or stenosis |
| Vasculitis | Lack of multifocal arterial narrowing or beading appearance |
| Basilar artery duplication | Complete separation of two basilar arteries along entire course |