Bell's Palsy¶
Summary
- Acute, unilateral facial nerve paralysis of unknown etiology
- Characterised by sudden onset of facial weakness, typically affecting one side of the face
- Diagnosis primarily clinical, with imaging used to rule out other causes
Pathophysiology¶
- Exact cause unknown, but believed to involve inflammation of the facial nerve (CN VII)
- Possible triggers include:
- Viral infections (e.g., herpes simplex virus, varicella-zoster virus)
- Immune-mediated processes
- Vascular ischaemia
- Inflammation leads to compression and oedema of the facial nerve within the facial canal
Demographics¶
- Annual incidence: 15-30 cases per 100,000 population
- Affects all age groups, but peak incidence in 15-45 years
- Slightly higher prevalence in:
- Pregnant women
- Patients with diabetes mellitus
- Individuals with upper respiratory tract infections
Diagnosis¶
- Primarily clinical, based on:
- Sudden onset of unilateral facial weakness
- Inability to close eye or wrinkle forehead on affected side
- Drooping of corner of mouth
- Physical examination:
- House-Brackmann scale to grade facial nerve function
- Assessment of taste and lacrimation
- Exclusion of other causes (e.g., stroke, tumour) through history and examination
Imaging¶
- Not routinely required for diagnosis
- May be used to rule out other causes or in cases of atypical presentation
- Modalities:
- MRI:
- T1-weighted with gadolinium: enhancement of the facial nerve
- FLAIR: hyperintensity of the facial nerve
- CT:
- Limited role in acute setting
- May show bony erosion in chronic cases
- Findings:
- Enhancement and swelling of the facial nerve, particularly in the labyrinthine and tympanic segments
- Normal brain parenchyma
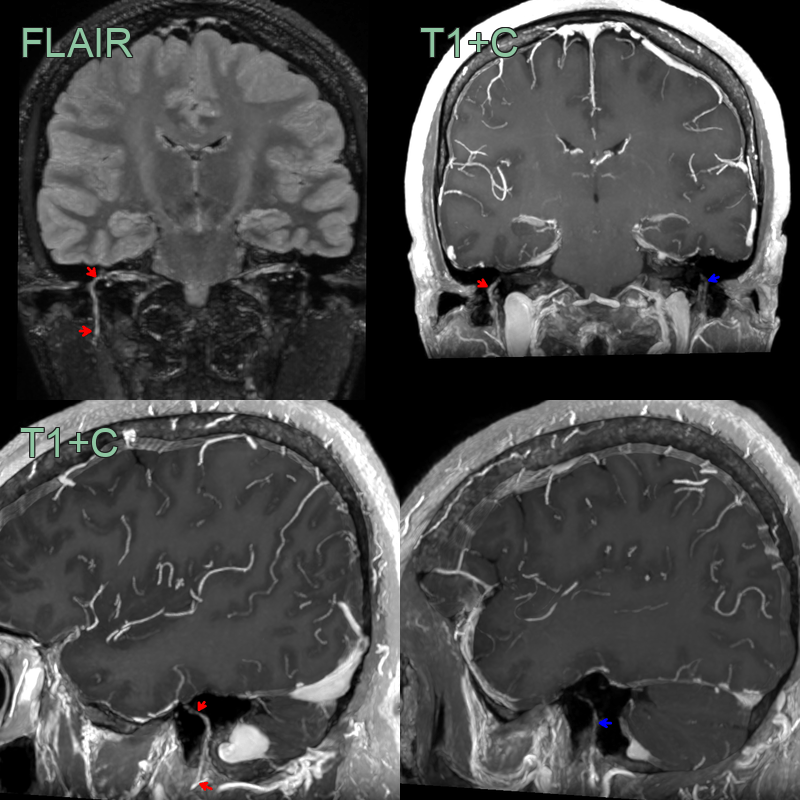
- 50-year-old patient presented with right sided facial weakness affecting the forehead.
- MRI showed a FLAIR hyperintensity, mild thickening, and pathological enhancement (labyrinthine, tympanic and mastoid segments; red arrow) of the right facial nerve and a normal left facial nerve (blue arrow).
Treatment¶
- Supportive care and medical management:
- Corticosteroids: Prednisone 60-80 mg daily for 5-7 days
- Antiviral therapy (e.g., valacyclovir) in combination with corticosteroids
- Eye care:
- Artificial tears and eye ointment
- Taping eyelid closed at night
- Physical therapy:
- Facial exercises to maintain muscle tone
- Surgical decompression:
- Reserved for severe cases or those with poor recovery
- Controversial and not routinely recommended
- Prognosis:
- 70-80% of patients recover completely within 3-6 months
- Poor prognostic factors: complete paralysis, age >60 years, hypertension, diabetes
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Stroke | Typically affects lower face only; other neurological deficits often present |
| Ramsay Hunt syndrome | Presence of vesicles in ear canal or on palate; severe otalgia |
| Vestibular schwannoma | Gradual onset; hearing loss; tinnitus; balance problems |
| Parotid gland tumour | Slow, progressive facial weakness; visible or palpable mass |
| Facial nerve trauma | History of facial injury or surgery |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy; lip swelling; fissured tongue |