Benign Parietal Thinning¶
Summary
- Benign parietal thinning is a focal thinning of the parietal bone, typically bilateral and symmetrical
- Asymptomatic condition, often discovered incidentally on imaging studies
- No intervention required; important to differentiate from pathological conditions
Pathophysiology¶
- Exact etiology remains unclear
- Hypothesized mechanisms:
- Congenital developmental variation
- Age-related bone resorption
- Hormonal influences, particularly in postmenopausal women
- Characterised by focal thinning of the outer table and diploe, with preservation of the inner table
Demographics¶
- More common in older adults, typically over 60 years of age
- Higher prevalence in females, particularly postmenopausal women
- No known racial or ethnic predisposition
- Estimated prevalence of 0.4-1.3% in the general population
Diagnosis¶
- Usually an incidental finding on imaging studies
- Clinical presentation:
- Asymptomatic
- No associated neurological deficits or palpable abnormalities
- Differential diagnosis:
- Metastatic lesions
- Multiple myeloma
- Hyperparathyroidism
- Fibrous dysplasia
- Paget's disease
Imaging¶
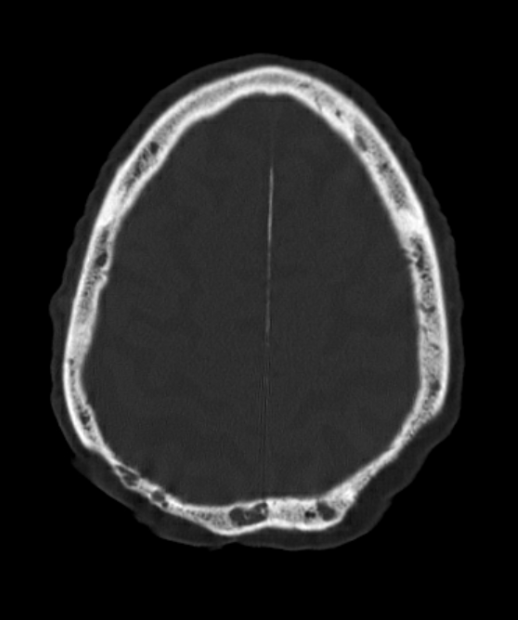
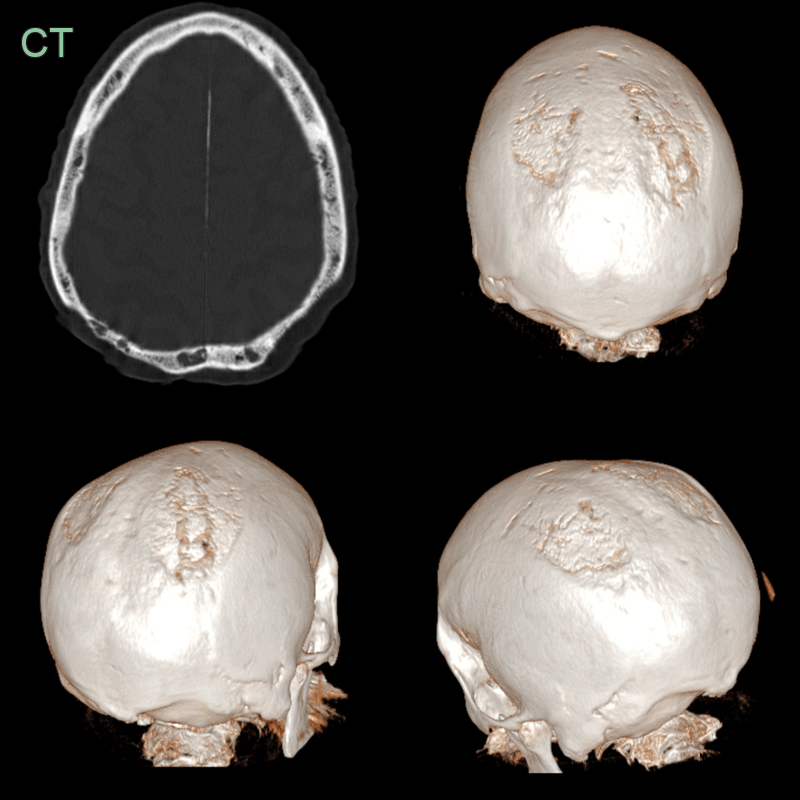
- CT:
- Bilateral, symmetrical focal thinning of the parietal bones
- Typically located in the parasagittal region
- Sharply demarcated margins
- Preservation of the inner table
- No associated soft tissue mass or bone destruction
- MRI:
- T1 and T2 signal intensity similar to normal bone marrow
- No contrast enhancement
- Skull radiographs:
- May show focal lucencies in the parietal region
- Less sensitive than CT for detection and characterization
- Incidental finding of thinning of the parietal bone with loss of the outer cortex that was stable over at least 5 years.
- The patient was systemically well with no clinical or labratory evidence of a hematological disorder.
Treatment¶
- No specific treatment required
- Patient reassurance and education about the benign nature of the condition
- Follow-up imaging may be considered in cases of diagnostic uncertainty
- Differentiation from pathological conditions is crucial to avoid unnecessary interventions
- Bone density screening may be recommended, particularly in postmenopausal women, to assess for concurrent osteoporosis
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Parietal skull fracture | Irregular, linear lucency without sclerotic margins; may be associated with intracranial haemorrhage |
| Lytic metastasis | Not symmetrical, irregular margins, associated soft tissue |
| Metastatic disease | Multiple lesions with destructive or permeative pattern; irregular margins; soft tissue component; no smooth bevelled edges |