Biotin Responsive Basal Ganglia Disease¶
Summary
- Rare neurometabolic disorder characterised by recurrent encephalopathy and bilateral basal ganglia lesions
- Caused by mutations in the SLC19A3 gene, affecting thiamine transport
- Responsive to biotin and thiamine supplementation, with potential for full recovery if treated early
Pathophysiology¶
- Autosomal recessive disorder caused by mutations in the SLC19A3 gene
- SLC19A3 encodes for thiamine transporter 2 (ThTR2)
- Impaired thiamine transport leads to:
- Mitochondrial dysfunction
- Energy depletion in basal ganglia and other brain regions
- Increased oxidative stress
- Biotin may act as a cofactor for carboxylases and enhance residual ThTR2 function
Demographics¶
- Rare disorder, with fewer than 100 cases reported worldwide
- Most commonly affects individuals of Arab descent
- Typically presents in childhood or adolescence
- No significant gender predilection
Diagnosis¶
- Clinical presentation:
- Recurrent episodes of encephalopathy
- Seizures
- Dystonia
- Ataxia
- Cognitive decline
- Laboratory findings:
- Normal serum thiamine levels
- Elevated lactate in cerebrospinal fluid (CSF)
- Genetic testing:
- Identification of biallelic mutations in SLC19A3 gene
Imaging¶
- MRI findings:
- Bilateral, symmetrical T2/FLAIR hyperintensities in basal ganglia
- Caudate nuclei
- Putamina
- Thalami
- Additional involvement may include:
- Cerebral cortex
- Brainstem
- Cerebellum
- MR spectroscopy:
- Elevated lactate peak in affected regions
- Follow-up imaging:
- Reversibility of lesions with treatment
- Potential for complete resolution if treated early
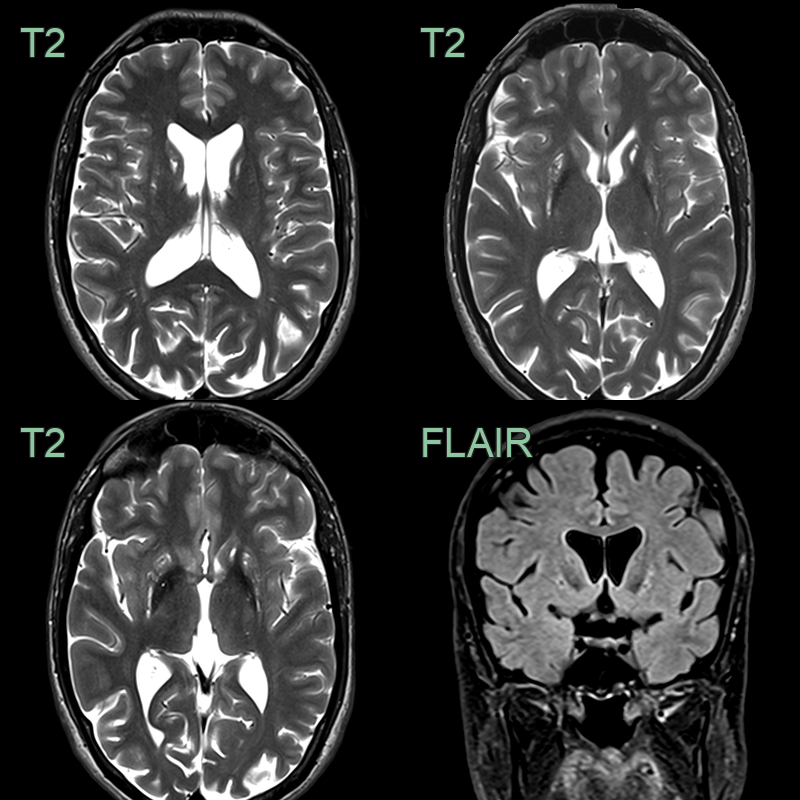
- 30-year-old patient with biotin related basal ganglia disease during acute presentation 20 years prior.
- MRI showed old gliotic damage and volume loss of the striatum basal ganglia.
Treatment¶
- Biotin supplementation:
- Typical dose: 5-10 mg/kg/day
- Thiamine supplementation:
- Typical dose: 50-100 mg/kg/day
- Combined biotin and thiamine therapy is more effective than biotin alone
- Early initiation of treatment is crucial for:
- Preventing neurological deterioration
- Reversing existing symptoms
- Improving long-term outcomes
- Lifelong supplementation is recommended
- Supportive care:
- Anticonvulsants for seizure control
- Physical and occupational therapy for motor symptoms
- Genetic counseling for affected families
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Leigh Syndrome | Typically earlier onset; lactate elevation in blood and CSF |
| Pantothenate Kinase-Associated Neurodegeneration | "Eye of the tiger" sign on T2-weighted MRI |
| Glutaric Aciduria Type 1 | Characteristic urine organic acid profile; macrocephaly |
| Carbon Monoxide Poisoning | History of exposure; carboxyhaemoglobin levels elevated |