Carasal¶
Summary
- Rare, benign, slow-growing tumour of the carotid body
- Typically presents as a painless, pulsatile mass in the lateral neck
- Characteristic "salt and pepper" appearance on CT and MRI imaging
Pathophysiology¶
- Arises from paraganglionic cells of the carotid body
- Located at the carotid bifurcation
- Highly vascularised tumour
- Usually non-functional, but may secrete catecholamines in rare cases
Demographics¶
- Peak incidence in 5th-6th decades of life
- Slight female predominance (1.5:1)
- Bilateral in 10-20% of cases
- Familial occurrence in 10% of cases, associated with genetic syndromes (e.g., MEN2, VHL)
Diagnosis¶
- Often asymptomatic, discovered incidentally
- Clinical presentation:
- Painless, slow-growing lateral neck mass
- Pulsatile on palpation
- May cause cranial nerve deficits (IX, X, XII) in advanced cases
- Biochemical testing:
- Plasma or urinary metanephrines if functional tumour suspected
- Biopsy generally contraindicated due to risk of haemorrhage
Imaging¶
- Ultrasound:
- Hypoechoic, well-defined mass at carotid bifurcation
- Splaying of internal and external carotid arteries ("lyre sign")
- Hypervascular on Doppler imaging
- CT:
- Avidly enhancing mass
- "Salt and pepper" appearance due to flow voids
- Splaying of carotid bifurcation
- MRI:
- T1: isointense to muscle
- T2: hyperintense with flow voids ("salt and pepper" appearance)
- Intense enhancement on post-contrast images
- Angiography:
- Hypervascular tumour blush
- Splaying of carotid bifurcation ("lyre sign")
- May be used for preoperative embolisation
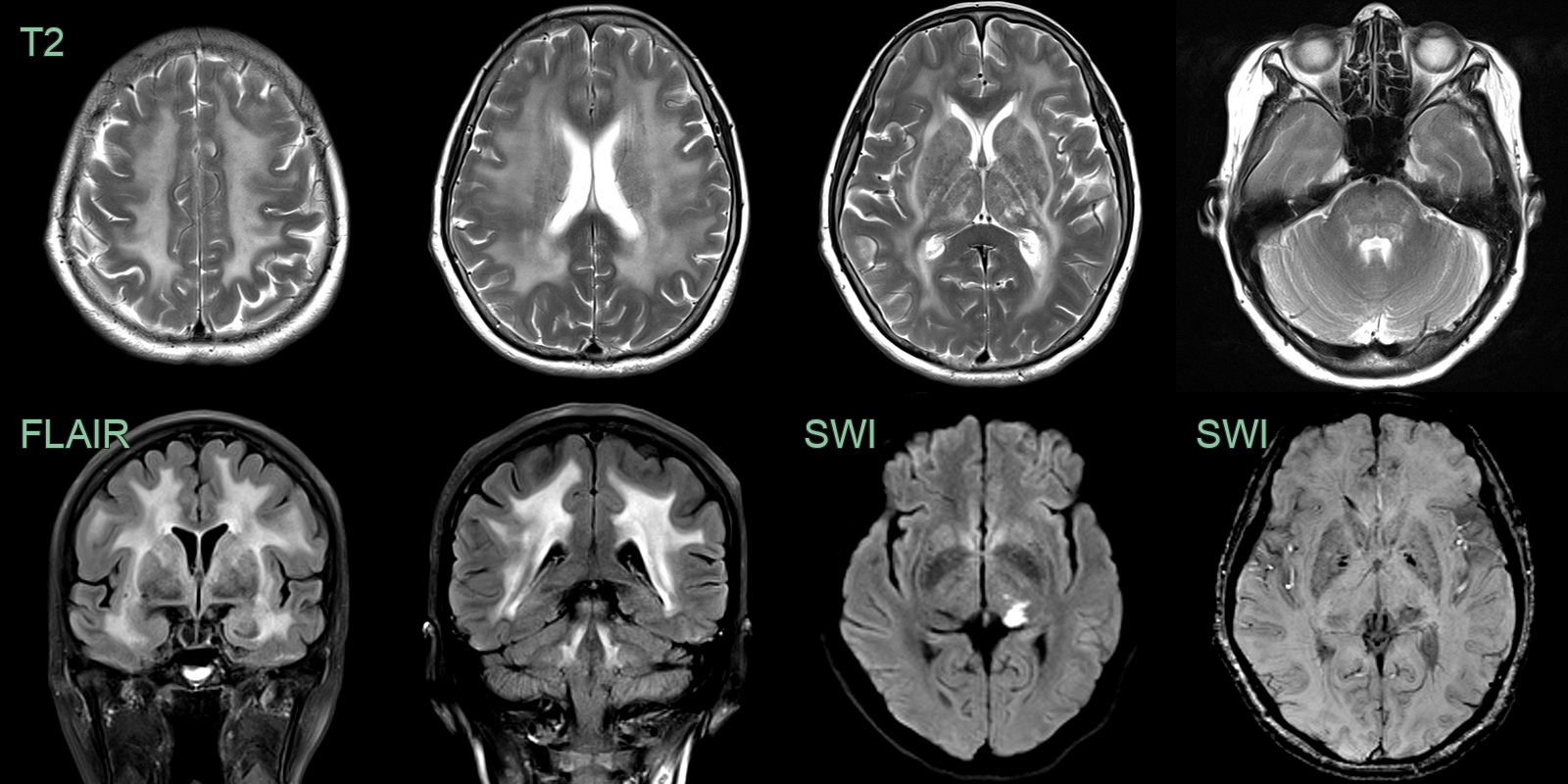
- A 50-year-old patient presented with a homonymous hemianopia and motor and sensory disturbance.
- MRI showed an acute left thalamic infarct on a background of a diffuse leukoencephalopathy affecting the cerebral and capsular white matter, the brainstem and superior cerebellar peduncles.
- There were no microhaemorrhages.
Treatment¶
- Surgical resection is the definitive treatment
- Preoperative embolisation may reduce intraoperative blood loss
- Radiotherapy for unresectable tumours or in elderly patients
- Regular follow-up due to risk of local recurrence
- Genetic counselling for familial cases
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| CADASIL | Anterior temporal lobe and external capsule white matter hyperintensities; NOTCH3 mutation; autosomal dominant; no anterior temporal pole sparing |
| CARASIL | Similar confluent white matter pattern; autosomal recessive; HTRA1 mutation; associated with early-onset spondylosis and alopecia |
| Hypertensive microangiopathy | Deep white matter and basal ganglia hyperintensities; associated with poorly controlled hypertension; lacks anterior temporal pole involvement |
| COL4A1-related small vessel disease | Deep cerebral microhaemorrhages; lacunar infarcts; porencephaly; COL4A1/COL4A2 mutations |
| MELAS | Stroke-like lesions not conforming to vascular territories; mitochondrial DNA mutations; elevated serum/CSF lactate |
| Cerebral amyloid angiopathy | Lobar microhaemorrhages; posterior predominance; cortical superficial siderosis; typically older patients |
| CSF1R-related leukoencephalopathy | Confluent white matter disease with calcifications on CT; thalamic involvement; CSF1R mutation |
| Susac syndrome | Corpus callosum "snowball" lesions at the central fibres; sensorineural hearing loss; branch retinal artery occlusions |