Carbon Monoxide Poisoning¶
Summary
- Carbon monoxide (CO) poisoning results from inhalation of CO gas, leading to tissue hypoxia
- Clinical presentation ranges from mild symptoms to coma and death
- Imaging findings are non-specific but may include hypodensities on CT and hyperintensities on MRI
Pathophysiology¶
- CO binds to haemoglobin with 200-250 times greater affinity than oxygen
- Forms carboxyhaemoglobin (COHb), reducing oxygen-carrying capacity of blood
- Causes leftward shift of oxyhaemoglobin dissociation curve, impairing oxygen delivery to tissues
- Direct cellular toxicity via inhibition of mitochondrial cytochrome c oxidase
Demographics¶
- Most common cause of fatal poisoning in many countries
- Higher incidence in winter months due to increased use of heating systems
- Risk factors:
- Faulty heating systems
- Enclosed spaces with poor ventilation
- Occupational exposure (e.g., firefighters, industrial workers)
Diagnosis¶
- Based on clinical suspicion and history of exposure
- Measurement of COHb levels in blood
- Normal: <3% in non-smokers, <10% in smokers
- Toxic levels: >10%
- Arterial blood gas analysis may show metabolic acidosis
- ECG may reveal ischaemic changes or arrhythmias
Imaging¶
- Brain CT:
- Acute: may be normal or show cerebral oedema
- Delayed: bilateral hypodensities in basal ganglia, particularly globus pallidus
- Brain MRI:
- T2-weighted and FLAIR: hyperintensities in basal ganglia, cerebral white matter, and hippocampus
- Diffusion-weighted imaging: restricted diffusion in affected areas
- Susceptibility-weighted imaging: may show petechial haemorrhages
- Chest radiograph:
- May be normal or show pulmonary oedema in severe cases
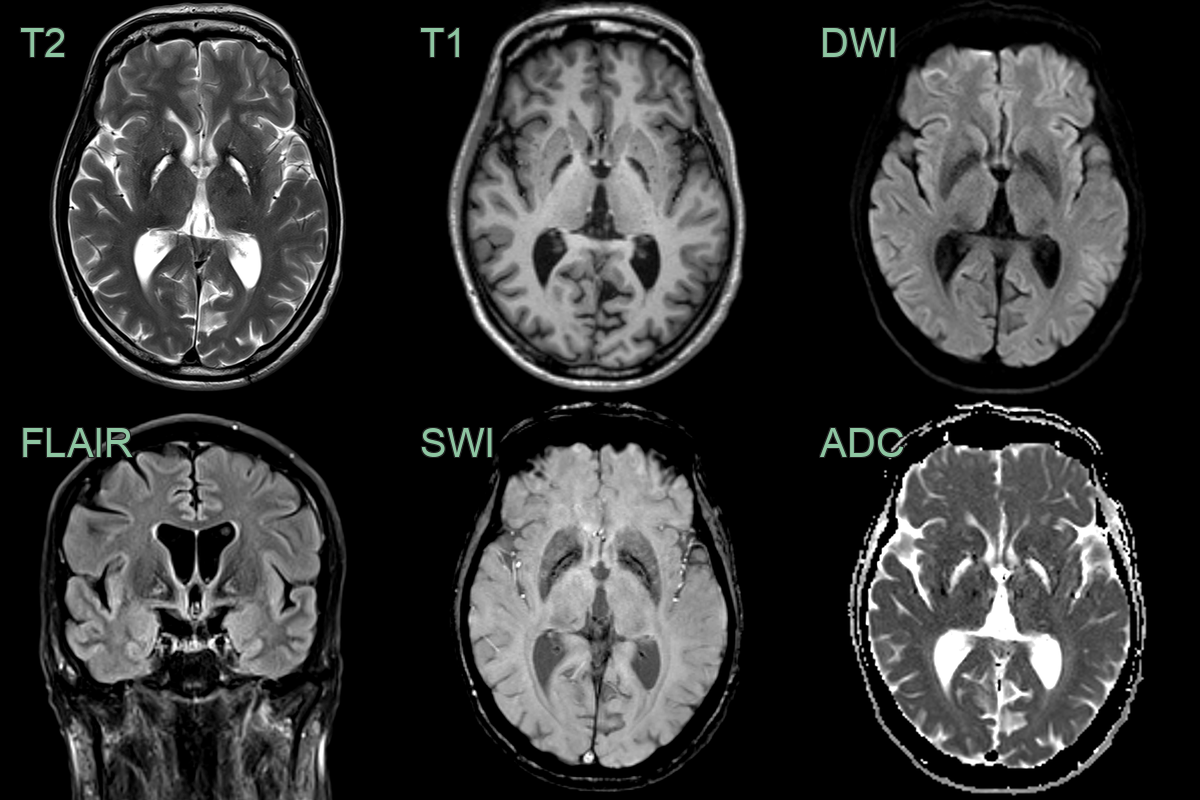
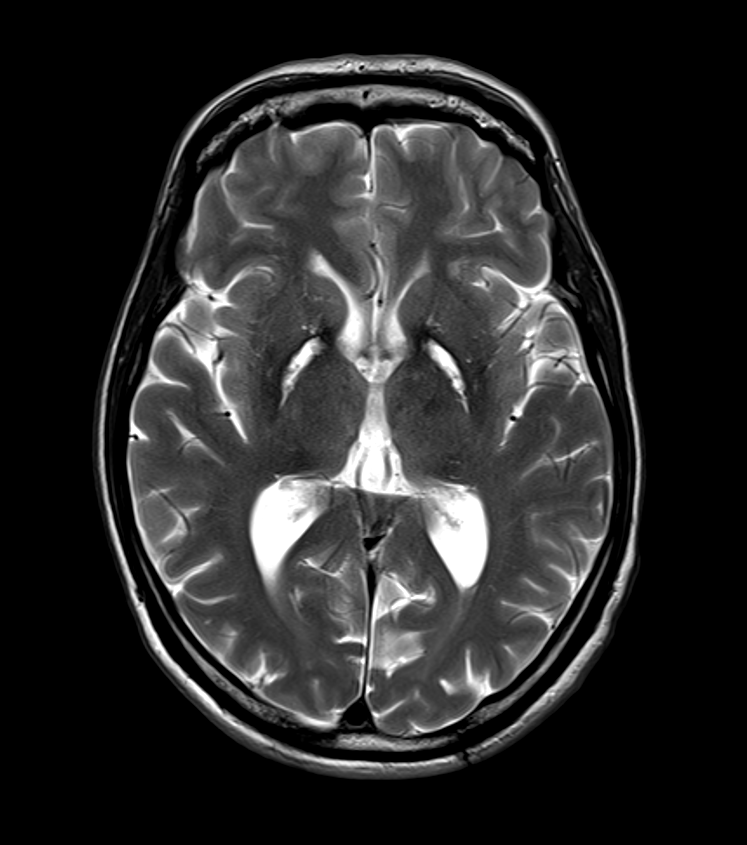
- A 50-year-old patient with a history of carbon monoxide exposure and extensive neuropsyhchiatric history.
- MRI showed gliosis and loss of volume of the globi pallidi bilaterally with a rim of susceptibility artefact, probably from siderosis.
- The appearances were consistent with the chronic manifestations of necrosis secondary to carbon monoxide poisoning.
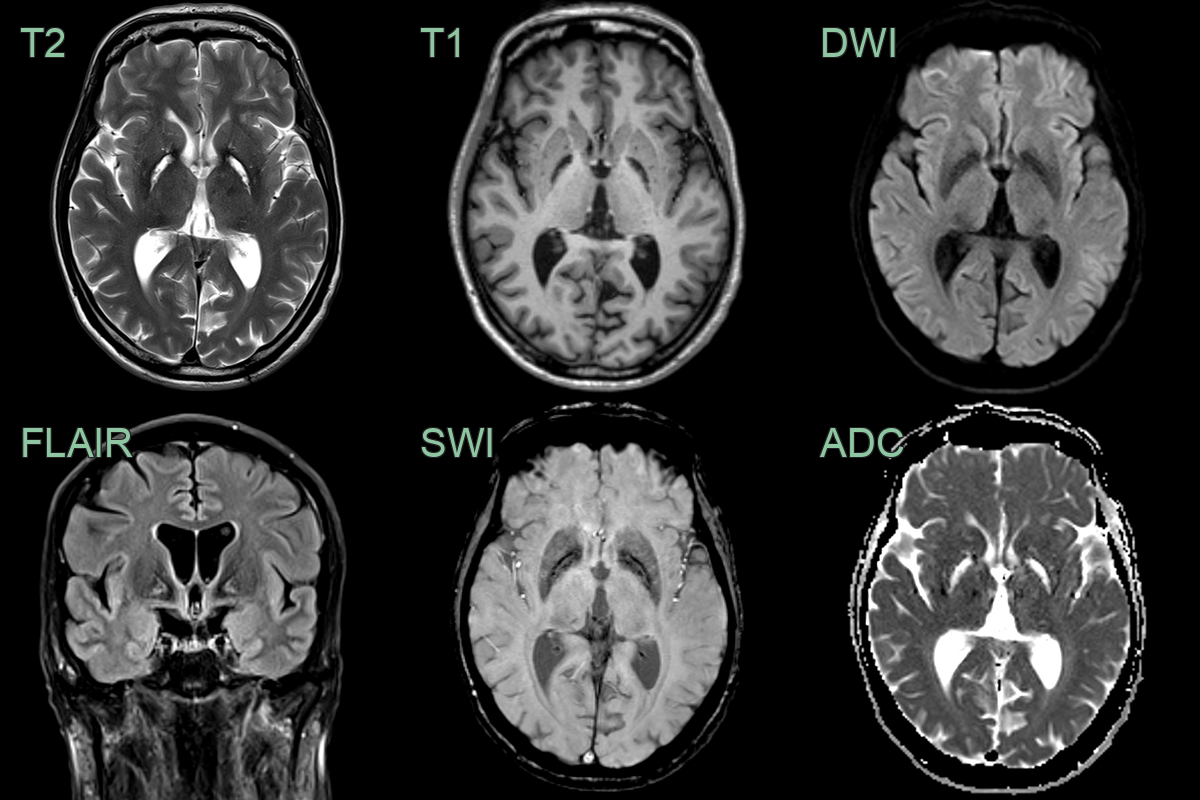
- A 50-year-old patient with a history of carbon monoxide exposure and extensive neuropsyhchiatric history.
- MRI showed gliosis and loss of volume of the globi pallidi bilaterally with a rim of susceptibility artefact, probably from siderosis.
- The appearances were consistent with the chronic manifestations of necrosis secondary to carbon monoxide poisoning.
Treatment¶
- Immediate removal from source of exposure
- High-flow oxygen therapy (100% oxygen via non-rebreather mask)
- Hyperbaric oxygen therapy in severe cases or pregnant patients
- Supportive care:
- Airway management
- Fluid resuscitation
- Correction of metabolic acidosis
- Monitoring for delayed neurological sequelae
- Long-term follow-up for cognitive and neurological deficits
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Hypoxic-ischaemic injury | Bilateral globus pallidus T2 hyperintensity with cortical and hippocampal involvement |
| Methanol toxicity | Bilateral putaminal necrosis with haemorrhage and optic nerve involvement |
| Osmotic demyelination | Central pontine T2 hyperintensity with extrapontine basal ganglia involvement |
| Japanese encephalitis | Bilateral thalamic and substantia nigra T2 hyperintensity |