Carotid Web¶
Summary
- Carotid web is a rare, non-atherosclerotic cause of ischaemic stroke
- Characterised by a shelf-like projection in the lumen of the internal carotid artery
- Diagnosis often challenging, requiring high-resolution imaging techniques
Pathophysiology¶
- Believed to be a variant of fibromuscular dysplasia
- Abnormal accumulation of fibrous tissue in the tunica intima of the carotid artery
- May act as a nidus for thrombus formation, leading to embolic stroke
- Typically located at the posterior wall of the carotid bulb or proximal internal carotid artery
Demographics¶
- More common in middle-aged adults (40-60 years)
- Higher prevalence in women
- Increased incidence in African American population
- Often associated with cryptogenic stroke in younger patients without traditional risk factors
Diagnosis¶
- Clinical presentation:
- Recurrent ischaemic strokes or transient ischaemic attacks
- Often misdiagnosed as cryptogenic stroke
- Physical examination:
- Usually unremarkable
- No specific findings associated with carotid web
Imaging¶
- Conventional angiography:
- Gold standard for diagnosis
- Appears as a thin, linear filling defect on the posterior wall of the carotid bulb
- CT angiography (CTA):
- High sensitivity and specificity for detection
- Axial images show a "shelf-like" filling defect
- Sagittal reconstructions demonstrate a characteristic "cobra head" appearance
- MR angiography (MRA):
- Less sensitive than CTA
- May show focal narrowing or filling defect in the carotid bulb
- Ultrasound:
- Limited utility due to low sensitivity
- May show a small, echogenic projection in the carotid lumen
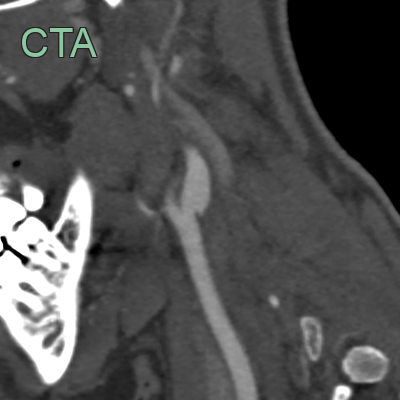
- Incidental finding of a linear filling defect along the posterior wall of the internal carotid artery.
Treatment¶
- Medical management:
- Antiplatelet therapy (e.g., aspirin, clopidogrel)
- Risk factor modification for stroke prevention
- Surgical intervention:
- Carotid endarterectomy: preferred treatment for symptomatic patients
- Carotid stenting: alternative option, especially for high-risk surgical candidates
- Endovascular therapy:
- Emerging treatment option
- Balloon angioplasty with or without stenting
- Follow-up:
- Regular imaging surveillance to monitor for recurrence or progression
- Long-term antiplatelet therapy may be necessary
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Atherosclerotic plaque | Carotid web appears as a thin, shelf-like filling defect on angiography, while atherosclerotic plaque is typically more irregular and eccentric |
| Fibromuscular dysplasia | Carotid web is typically located at the carotid bulb, while fibromuscular dysplasia affects more distal segments of the carotid artery |
| Carotid dissection | Carotid web is a static lesion, while dissection may show a dynamic intimal flap or double lumen on imaging |
| Carotid artery spasm | Carotid web is a persistent finding, whereas spasm is transient and can be relieved with vasodilators |
| Intraluminal thrombus | Carotid web has a characteristic shelf-like appearance, while thrombus typically appears as a filling defect without the shelf-like morphology |
| Carotid body tumour | Carotid web does not enhance on contrast imaging, while carotid body tumours typically show intense enhancement |
| Arteritis | Carotid web is localised, while arteritis often involves longer segments of the vessel and may show wall thickening |
| Pseudoaneurysm | Carotid web does not expand the vessel lumen, unlike a pseudoaneurysm which appears as an outpouching |