Cauda Equina Compression¶
Summary
- Compression of nerve roots below L1-L2 spinal level
- Caused by space-occupying lesions in the spinal canal
- Presents with lower back pain, saddle anesthesia, and bladder/bowel dysfunction
Pathophysiology¶
- Compression of lumbosacral nerve roots within the spinal canal
- Common causes:
- Herniated lumbar disc (most frequent)
- Spinal stenosis
- Tumour (primary or metastatic)
- Trauma
- Epidural abscess or haematoma
- Leads to ischaemia and potential permanent nerve damage if not treated promptly
Demographics¶
- Incidence: 1-3 cases per 100,000 population per year
- Most common in adults aged 30-50 years
- Slightly more prevalent in males
- Risk factors:
- Degenerative disc disease
- History of spinal surgery
- Spinal trauma
- Coagulopathies (for epidural haematoma)
Diagnosis¶
- Clinical presentation:
- Low back pain
- Bilateral sciatica
- Saddle anesthesia
- Bladder and/or bowel dysfunction
- Lower extremity weakness
- Physical examination:
- Reduced perianal sensation
- Decreased anal sphincter tone
- Lower extremity motor and sensory deficits
- Diagnostic criteria:
- One or more of: bladder/bowel dysfunction, reduced sensation in saddle area, sexual dysfunction
- Plus one or more of: low back pain, bilateral sciatica, lower extremity sensorimotor deficits
Imaging¶
- MRI:
- Gold standard for diagnosis
- T1-weighted: assess vertebral body alignment and marrow changes
- T2-weighted: evaluate disc herniations, spinal cord, and nerve root compression
- Gadolinium-enhanced: useful for detecting tumours or infections
- CT myelography:
- Alternative when MRI is contraindicated
- Shows compression of nerve roots and thecal sac
- Plain radiographs:
- Limited utility, may show vertebral body misalignment or fractures
- CT:
- Useful for assessing bony abnormalities and fractures
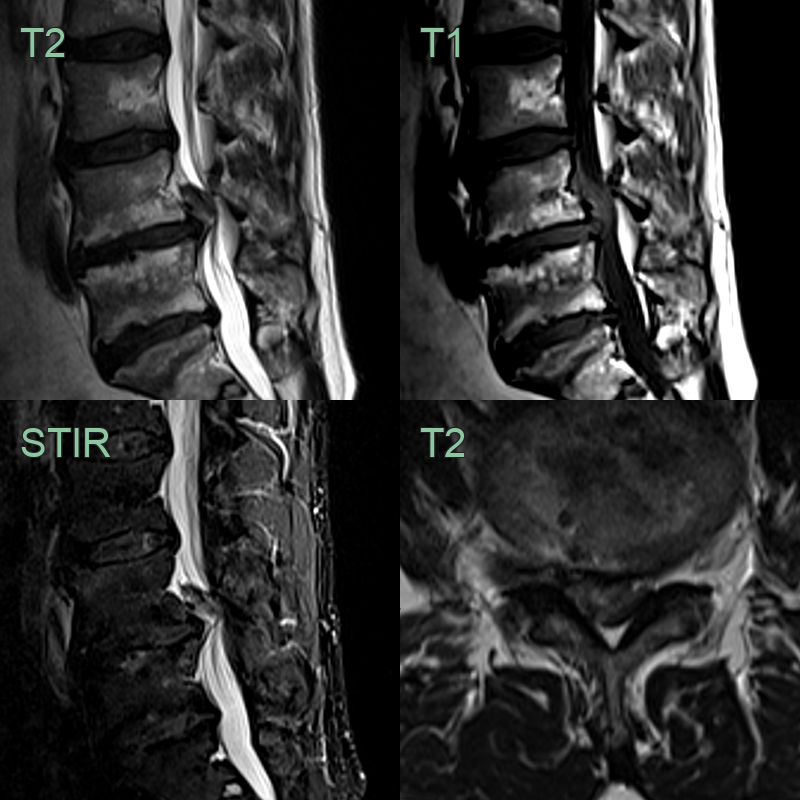
- 50-year-old patient presented with acute onset severe sciatica.
- At L4-5, a cranially migrated disc extrusion caused effacement of all CSF and compression of the cauda equina.
Treatment¶
- Emergency surgical decompression:
- Indicated for most cases, especially with progressive neurological deficits
- Ideally performed within 48 hours of symptom onset for best outcomes
- Surgical approaches:
- Laminectomy and discectomy for disc herniation
- Laminectomy and tumour resection for spinal tumours
- Drainage and antibiotics for epidural abscess
- Conservative management:
- Reserved for select cases with minimal symptoms or high surgical risk
- Includes bed rest, pain management, and close neurological monitoring
- Post-operative care:
- Physical therapy and rehabilitation
- Regular follow-up to assess neurological recovery
- Prognosis:
- Depends on the duration of symptoms before treatment
- Early intervention associated with better outcomes
- Some patients may have residual neurological deficits despite treatment
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Lumbar Disc Herniation | Usually affects single nerve root; no bowel/bladder dysfunction |
| Spinal Stenosis | Gradual onset; symptoms worsen with extension and improve with flexion |
| Conus Medullaris Syndrome | Higher level of neurological deficit (T12-L1); symmetric symptoms |
| Peripheral Neuropathy | Gradual onset; typically symmetrical; no back pain |
| Guillain-Barré Syndrome | Enhancement of spinal nerve roots on post-contrast MRI; anterior predominant root involvement |
| Multiple Sclerosis | Brain lesions on MRI; short spinal cord lesion; no mass lesion at cauda equina |
| Spinal Cord Tumour | Intramedullary or intradural extramedullary mass with enhancement; expansile cord |
| Epidural Abscess | Rim-enhancing epidural collection on MRI; end-plate erosion if discitis present |
| Transverse Myelitis | Intramedullary T2 signal without compressive mass; cord expansion |
| Aortic Dissection | Aortic lumen with intimal flap on CT; no intraspinal mass |