Cerebral Amyloid Angiopathy-Related Inflammation (CAA-ri)¶
Summary
- CAA-ri is a rare inflammatory variant of cerebral amyloid angiopathy
- Characterised by acute to subacute onset of headache, cognitive decline, seizures, and focal neurological deficits
- MRI typically shows asymmetric white matter hyperintensities, microbleeds, and leptomeningeal enhancement
Pathophysiology¶
- Inflammatory response to β-amyloid deposits in cerebral vessel walls
- Two proposed mechanisms:
- Autoimmune response against amyloid-β
- Excessive clearance of amyloid-β by activated microglia
- Associated with APOE ε4/ε4 genotype
Demographics¶
- Rare condition, exact prevalence unknown
- Typically affects older adults (mean age 67 years)
- No clear gender predilection
Diagnosis¶
- Clinical presentation:
- Acute to subacute onset of symptoms
- Headache, cognitive decline, seizures, focal neurological deficits
- Diagnostic criteria (all required) :
- Acute/subacute onset of symptoms
- Age ≥40 years
- ≥1 of: headache, decreased consciousness, behavioural change, focal neurological signs
- MRI findings consistent with CAA-ri
- Absence of neoplastic, infectious, or other cause
Imaging¶
- MRI findings:
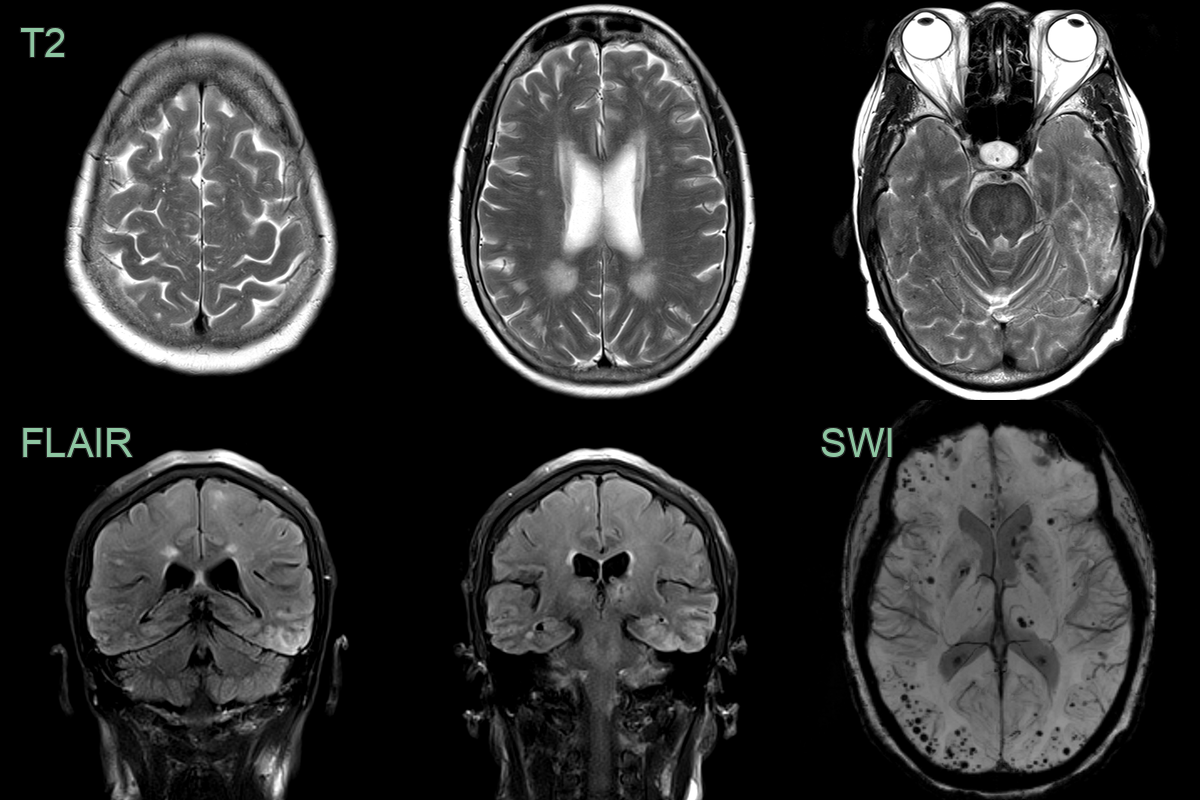
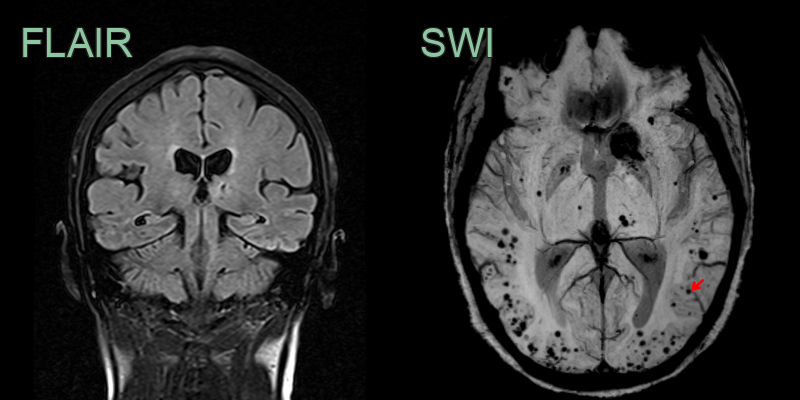
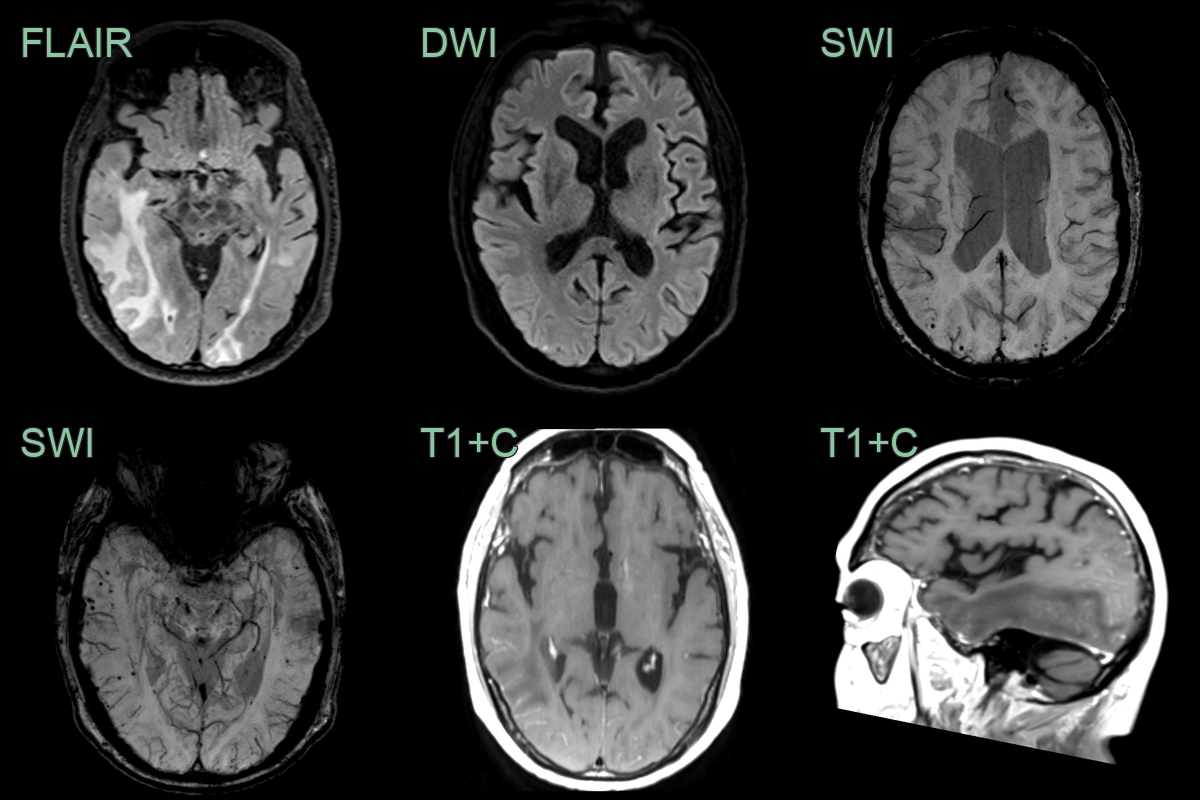
- Asymmetric white matter hyperintensities on T2/FLAIR
- Microbleeds on susceptibility-weighted imaging (SWI)
- Cortical superficial siderosis
- Leptomeningeal enhancement
- Lobar microbleeds or lobar haemorrhages
- CT findings:
- Hypodensities in affected white matter
- May show lobar haemorrhages
Treatment¶
- No standardized treatment protocol
- Immunosuppressive therapy:
- High-dose corticosteroids (e.g., methylprednisolone)
- Cyclophosphamide or methotrexate in refractory cases
- Supportive care:
- Antiepileptic drugs for seizure control
- Cognitive rehabilitation
- Monitoring:
- Regular clinical and radiological follow-up
- Assess for recurrence and treatment response
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Multiple Sclerosis | Ovoid periventricular and callosal lesions; Dawson's fingers on sagittal FLAIR; no cortical microbleeds or siderosis |
| Acute Disseminated Encephalomyelitis (ADEM) | Diffuse bilateral white matter T2 signal with basal ganglia involvement; no microbleeds or siderosis |
| Primary CNS Vasculitis | Multifocal cortical and subcortical infarcts; vessel wall enhancement on high-resolution MRI; no cortical microbleeds |
| Posterior Reversible Encephalopathy Syndrome (PRES) | Posterior-predominant vasogenic oedema with elevated ADC; no microbleeds; resolves on follow-up |
| Gliomatosis cerebri / High-grade glioma | Infiltrating T2 signal abnormality with mass effect; enhancement in high-grade tumours; no lobar microbleeds |
| Cerebral Abscess | Thin smooth ring-enhancing lesion with restricted DWI; surrounding vasogenic oedema; no siderosis |
| Progressive Multifocal Leukoencephalopathy (PML) | Subcortical U-fibre involvement; no enhancement or mass effect; restricted diffusion at active edge; no microbleeds |
| Acute Ischaemic Stroke | Wedge-shaped DWI restriction following vascular territory; no microbleeds or leptomeningeal enhancement |
| Cerebral Venous Thrombosis | Filling defects in venous sinuses on CT/MR venography; venous infarcts crossing arterial territories |
| Creutzfeldt-Jakob Disease | Cortical ribboning and basal ganglia DWI restriction; pulvinar sign on T2; no microbleeds |