Cerebral metastasis¶
Summary
- Cerebral metastases are secondary brain tumours originating from primary cancers elsewhere in the body
- Most common in lung cancer, breast cancer, and melanoma patients
- Typically present with neurological symptoms, headaches, and seizures
Pathophysiology¶
- Metastatic spread occurs via:
- Hematogenous dissemination (most common)
- Direct extension from adjacent structures
- Lymphatic spread (rare)
- Tumour cells breach the blood-brain barrier and proliferate in brain parenchyma
- Growth factors and angiogenesis promote tumour expansion
Demographics¶
- Incidence:
- 20-40% of cancer patients develop brain metastases
- Increasing due to improved systemic therapies and longer patient survival
- Most common primary sites:
- Lung cancer (40-50%)
- Breast cancer (15-25%)
- Melanoma (5-20%)
- Colorectal cancer (5-10%)
- Renal cell carcinoma (5-10%)
Diagnosis¶
- Clinical presentation:
- Headache (40-50%)
- Focal neurological deficits (20-40%)
- Cognitive changes (30-35%)
- Seizures (10-20%)
- Diagnostic workup:
- Neurological examination
- Contrast-enhanced MRI (gold standard)
- CT scan (if MRI contraindicated)
- Biopsy (if primary cancer unknown or atypical presentation)
Imaging¶
- MRI findings:
- T1-weighted: iso- to hypointense lesions
- T2-weighted: iso- to hyperintense lesions
- T1 post-contrast: ring-enhancing or nodular enhancement
- Surrounding vasogenic oedema on T2/FLAIR
- CT findings:
- Hypodense or isodense lesions
- Heterogeneous enhancement with contrast
- Calcifications (rare)
- Advanced imaging techniques:
- Perfusion imaging: increased relative cerebral blood volume
- Spectroscopy: elevated choline, reduced N-acetylaspartate
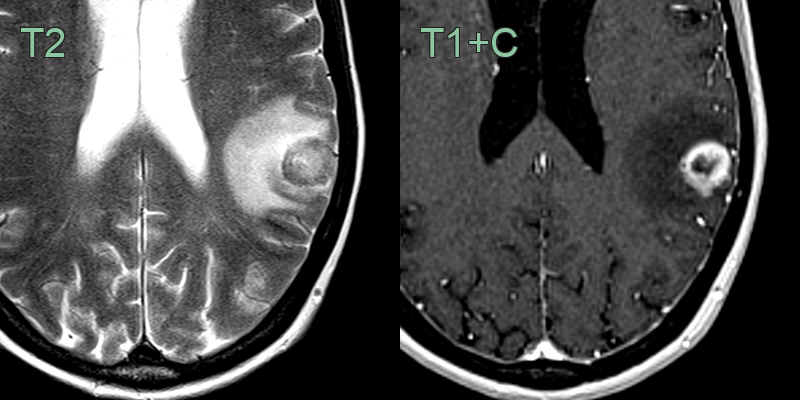
- A 60-year-old patient presented with right sided weakness.
- MRI showed a ring-enhancing lesion near grey-white matter interface with surrounding vasogenic oedema.
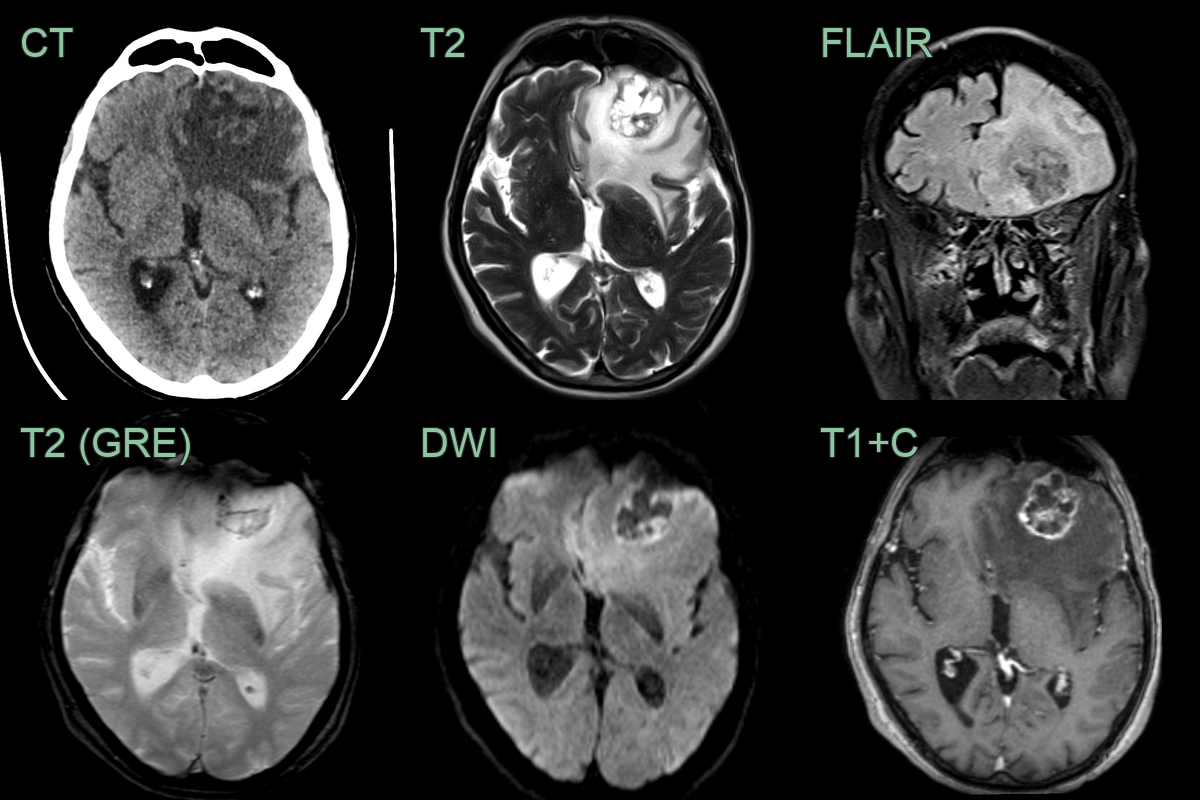
- A 80-year-old patient with a history of bladder cancer presented with headche.
- Imaging showed a peripherally enhancing lesion containing blood product in the left frontal lobe with a large volume of surrounding vasogenic oedema.
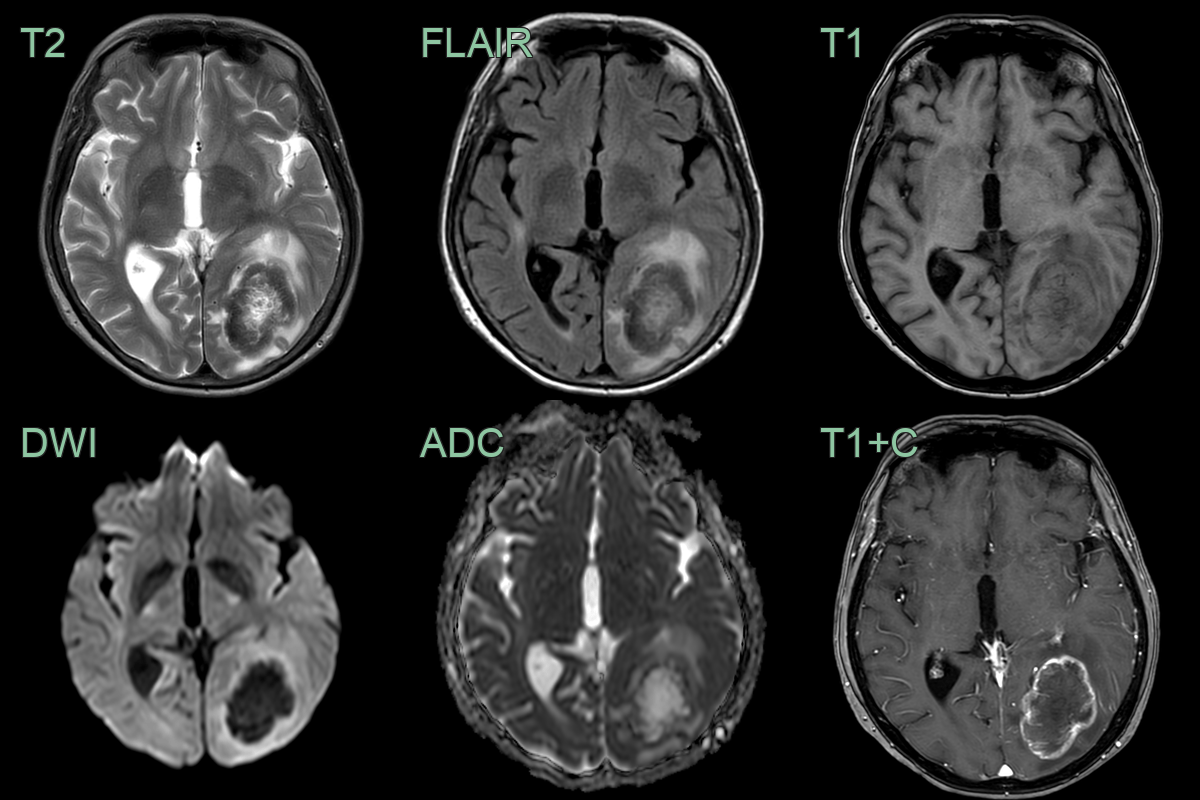
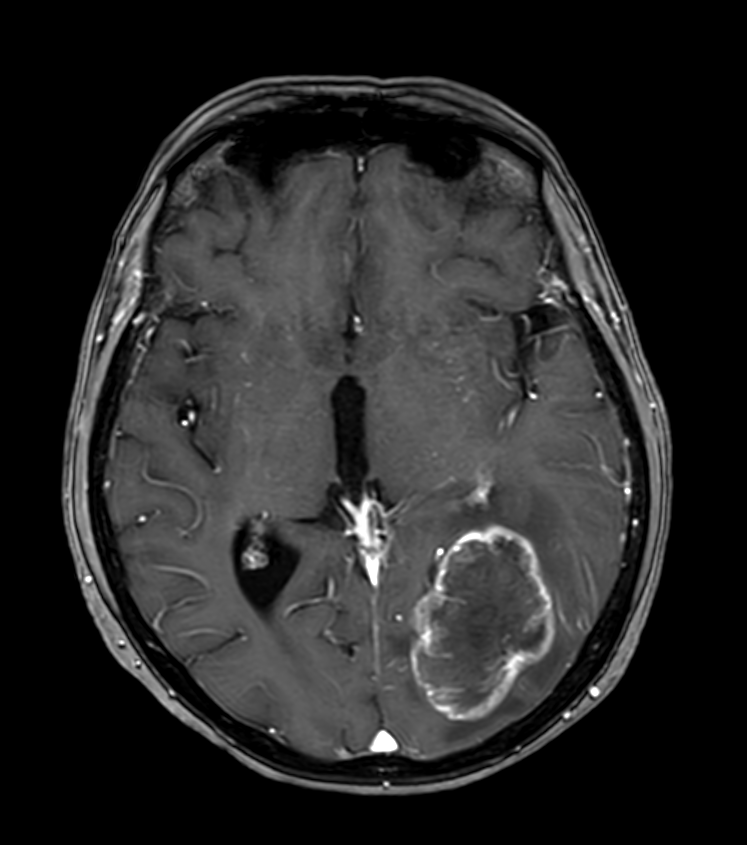
- A 60-year-old patient who was diagnosed with colonic cancer three years prior presented with a right visual field defect and headache.
- A large left occipital lobe lesion showed peripheral enhancement and was surrounded by vasogenic oedema.
- The peripheral T2-hypointensity within the lesion has been reported to be related to collagen accumulation.
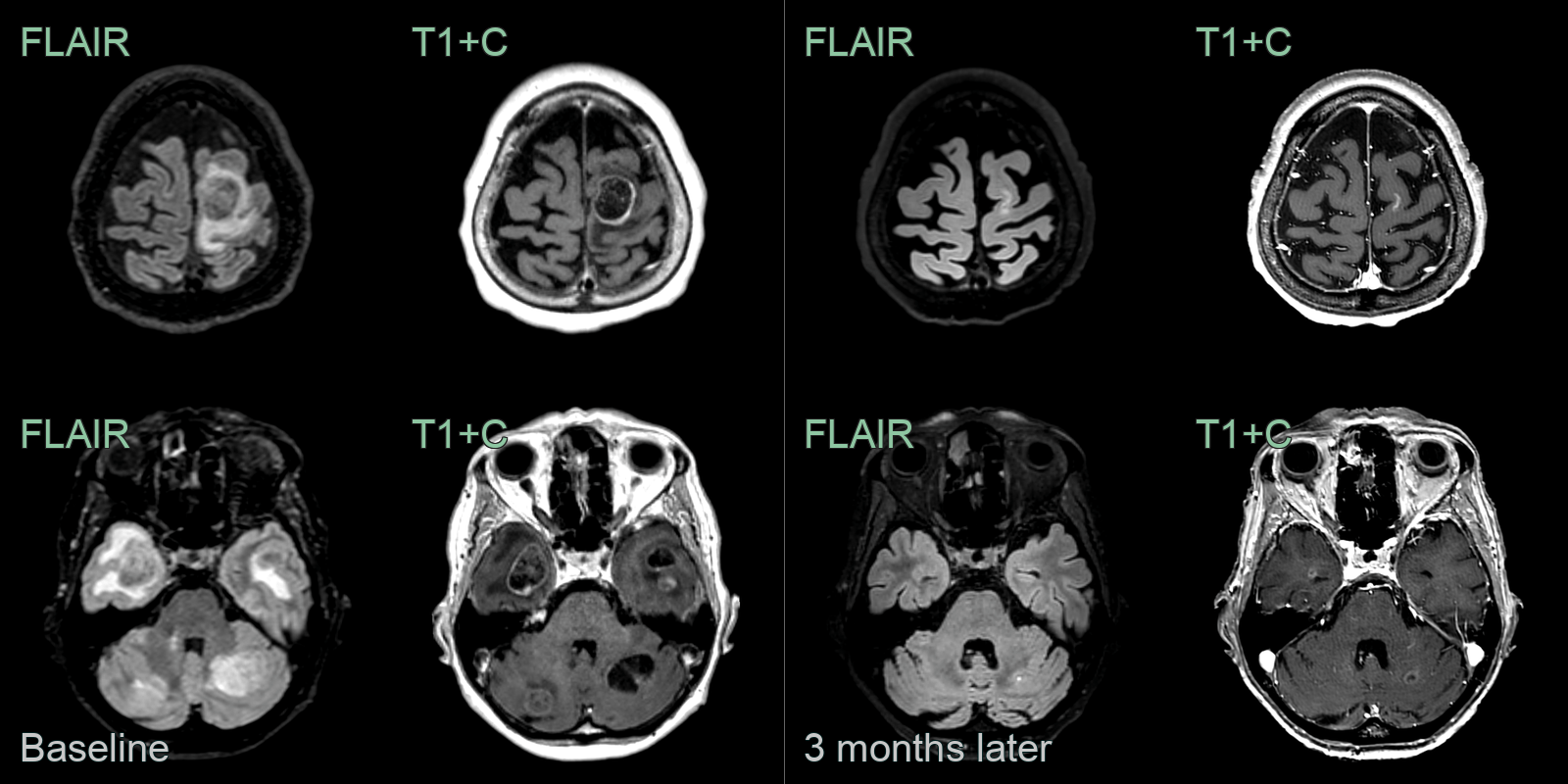
- A 70-year-old patient with small cell lung cancer presented with right leg weakness.
- MRI showed many peripherally enhancing lesions, the larges of which was in the left paracentral lobule.
- Following chemotherapy, MRI showed a marked reduction in the size of all of the lesions and the surrounding oedema.
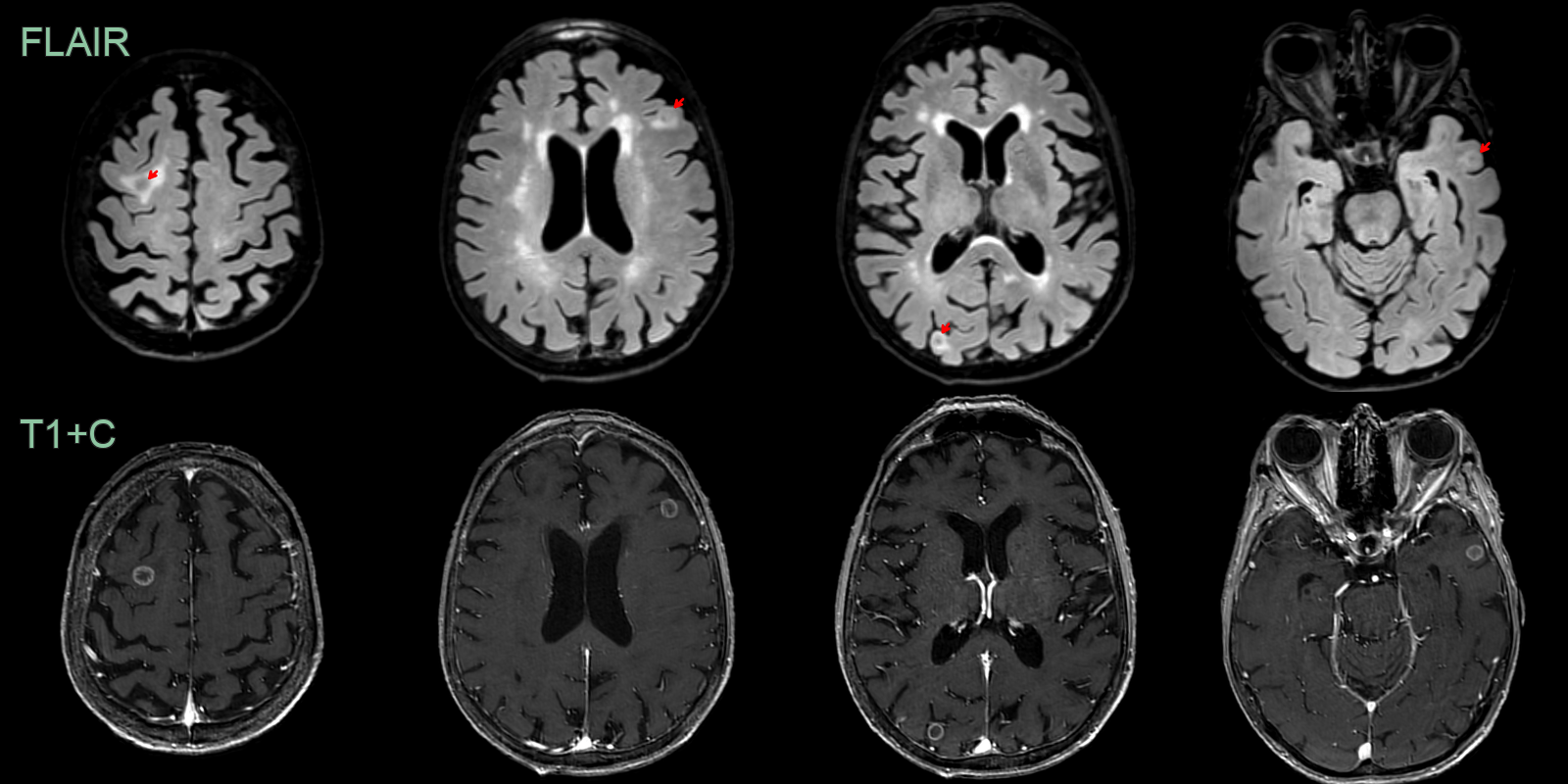
 * 70-year-old patient with a new diagnosis of non-small cell lung cancer had an MRI to 'screen' for metastasis.
* MRI showed subcentrimeter ring-enhancing lesions with variable amounts of surrounding vasogenic oedema.
* 70-year-old patient with a new diagnosis of non-small cell lung cancer had an MRI to 'screen' for metastasis.
* MRI showed subcentrimeter ring-enhancing lesions with variable amounts of surrounding vasogenic oedema.
Treatment¶
- Multidisciplinary approach:
- Neurosurgery
- Radiation oncology
- Medical oncology
- Treatment options:
- Surgical resection:
- For accessible, large (>3 cm) solitary lesions
- Improves local control and survival
- Stereotactic radiosurgery (SRS):
- For small (<3 cm) or multiple lesions
- High-dose, focused radiation
- Whole-brain radiation therapy (WBRT):
- For multiple lesions or leptomeningeal disease
- Associated with cognitive decline
- Systemic therapy:
- Chemotherapy
- Targeted therapies (e.g., EGFR inhibitors for lung cancer)
- Immunotherapy (e.g., checkpoint inhibitors for melanoma)
- Supportive care:
- Corticosteroids for oedema management
- Anticonvulsants for seizure control
- Pain management
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Primary brain tumour (high-grade glioma) | Usually single lesion with infiltrative margins crossing white matter tracts; no grey-white junction predilection |
| Cerebral abscess | Thin smooth ring enhancement with restricted diffusion centrally; may have satellite lesions |
| Multiple sclerosis | Ovoid periventricular lesions, often with "Dawson's fingers" on sagittal FLAIR; no surrounding vasogenic oedema |
| Cerebral infarction | Follows vascular territory; wedge-shaped; diffusion restriction in acute phase; cortical gyral enhancement |
| Glioblastoma | Single lesion with central necrosis and irregular ring enhancement; crosses corpus callosum; more infiltrative margins |
| Lymphoma | Periventricular location; homogeneous enhancement; restricted diffusion; hyperdense on non-contrast CT |
| Toxoplasmosis | Multiple ring-enhancing lesions; basal ganglia predilection; eccentric nodule ("target sign") |
| Radiation necrosis | Located within prior radiation field; identical ring enhancement; MR perfusion/spectroscopy may help distinguish |
| Neurocysticercosis | Cystic lesions with eccentric scolex nodule; perilesional calcification; no grey-white junction predilection |
| Tuberculoma | Conglomerate ring-enhancing lesions; central T2 hypointensity; leptomeningeal enhancement |