Cerebral Microhaemorrhages¶
Summary
- Small (< 10 mm) haemorrhages in the brain parenchyma
- Associated with cerebral amyloid angiopathy, hypertensive arteriopathy, and other vascular pathologies
- Detected on susceptibility-weighted MRI sequences as small, round hypointensities
Pathophysiology¶
- Result from rupture of small vessels, typically arterioles or capillaries
- Common aetiologies:
- Cerebral amyloid angiopathy (CAA): amyloid-β deposition in vessel walls
- Hypertensive arteriopathy: lipohyalinosis and fibrinoid necrosis of small vessels
- Diffuse axonal injury in traumatic brain injury
- Chronic hypertension leads to arteriolosclerosis and increased risk of microhaemorrhages
- CAA-related microhaemorrhages typically occur in lobar regions
- Hypertensive microhaemorrhages often found in deep brain structures and brainstem
Demographics¶
- Prevalence increases with age
- More common in:
- Elderly population (>60 years)
- Patients with hypertension
- Individuals with cerebrovascular disease
- Patients with Alzheimer's disease or vascular dementia
- Higher prevalence in Asian populations compared to Caucasians
Diagnosis¶
- Often asymptomatic and discovered incidentally on neuroimaging
- Clinical presentation may include:
- Cognitive decline
- Increased risk of future intracerebral haemorrhage
- Possible contribution to gait disturbances and falls
- Neurological examination typically normal
- Cognitive assessment may reveal subtle deficits in executive function or processing speed
Imaging¶
- Best detected on MRI using susceptibility-weighted imaging (SWI) or T2*-weighted gradient-echo sequences
- Appearance:
- Small (< 10 mm), round, hypointense foci on SWI or T2*
- "Blooming" effect due to paramagnetic properties of haemosiderin
- Distribution:
- Lobar: suggestive of CAA
- Deep/infratentorial: suggestive of hypertensive arteriopathy
- Microbleed Anatomical Rating Scale (MARS) used for standardised reporting
- CT imaging: generally not sensitive for detecting microhaemorrhages
- Differential diagnosis:
- Calcifications
- Flow voids in small vessels
- Cavernous malformations
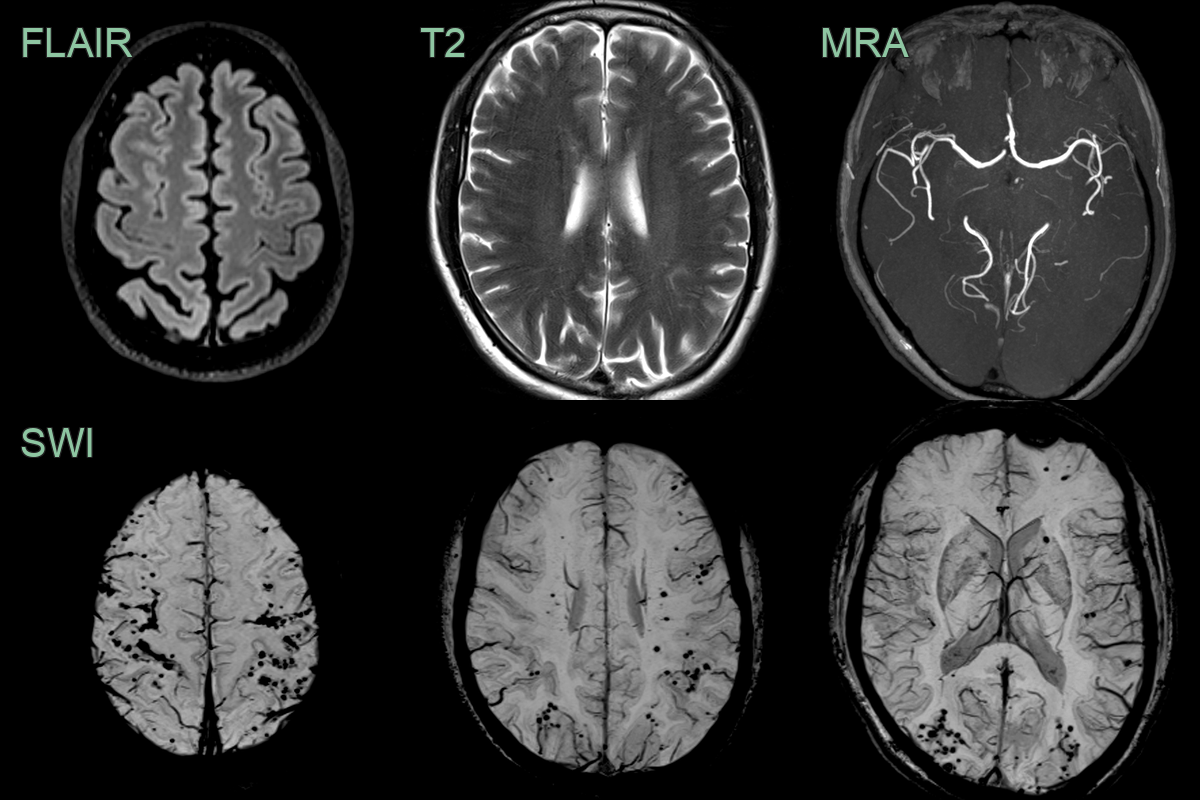
- A 50-year-old patient with a known atrial myxoma presented following a sensory TIA.
- MRI showed mainly peripheral cerebral microhaemorrhages - some appeared to be cortical or subpial.
Treatment¶
- No specific treatment for microhaemorrhages themselves
- Management focuses on underlying causes and risk factor modification:
- Strict blood pressure control for hypertensive arteriopathy
- Anticoagulation management:
- Careful consideration in patients with numerous microhaemorrhages
- Potential increased risk of intracerebral haemorrhage with anticoagulants
- Lifestyle modifications:
- Smoking cessation
- Alcohol moderation
- Regular exercise
- Cognitive rehabilitation for patients with associated cognitive decline
- Regular follow-up imaging to monitor progression
- Future therapeutic targets:
- Anti-amyloid therapies for CAA-related microhaemorrhages
- Neuroprotective agents to reduce oxidative stress and inflammation
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Cavernous malformations | Larger size, "popcorn" appearance on T2-weighted MRI |
| Cerebral amyloid angiopathy | Predominantly lobar distribution, associated with cognitive decline |
| Hypertensive microangiopathy | Deep brain location (basal ganglia, thalamus, pons) |
| Cerebral metastases | Larger size; surrounding vasogenic oedema; grey-white junction location; nodular or ring enhancement |
| Multiple sclerosis | Ovoid periventricular lesions; "Dawson's fingers" on sagittal FLAIR; no GRE/SWI blooming |
| Neurocysticercosis | Cystic appearance with eccentric scolex nodule; calcifications; GRE blooming without haemosiderin pattern |
| Radiation-induced vasculopathy | Confined to prior radiation field; may have associated white matter signal change |
| Septic emboli | Multiple small infarcts with restricted DWI; some lesions may have central restricted diffusion |
| Vasculitis | Beaded appearance of vessels on angiography |