Cerebral Proliferative Angiopathy (CPA)¶
Summary
- Rare vascular malformation characterised by diffuse network of abnormal vessels
- Distinct from classical arteriovenous malformations (AVMs)
- Presents with headaches, seizures, or focal neurological deficits
Pathophysiology¶
- Diffuse vascular abnormality with interposed normal brain parenchyma
- Angiogenesis likely plays a key role in pathogenesis
- Lack of large arteriovenous shunts, unlike classical AVMs
- Associated with chronic cerebral ischaemia and neoangiogenesis
Demographics¶
- Rare condition, exact prevalence unknown
- Typically affects younger patients (mean age 22 years)
- Female predominance (2:1 female to male ratio)
- No clear genetic or hereditary component identified
Diagnosis¶
- Clinical presentation:
- Headaches (most common)
- Seizures
- Focal neurological deficits
- Rarely, intracranial haemorrhage
- Differential diagnosis:
- Classical AVM
- Moyamoya disease
- Sturge-Weber syndrome
- Diagnosis confirmed by characteristic imaging findings
Imaging¶
- CT:
- Diffuse, enhancing vascular network
- Absence of large nidus or dominant feeding arteries
- MRI:
- T1: Diffuse hypointense signal
- T2: Flow voids and hyperintense interposed brain tissue
- Susceptibility-weighted imaging (SWI): Prominent vascular network
- Angiography:
- "Puffy, cloudy" appearance of abnormal vessels
- Absence of early venous drainage
- Capillary blush in late arterial phase
- Perfusion studies:
- Decreased cerebral blood flow in affected regions
- Increased mean transit time and time to peak
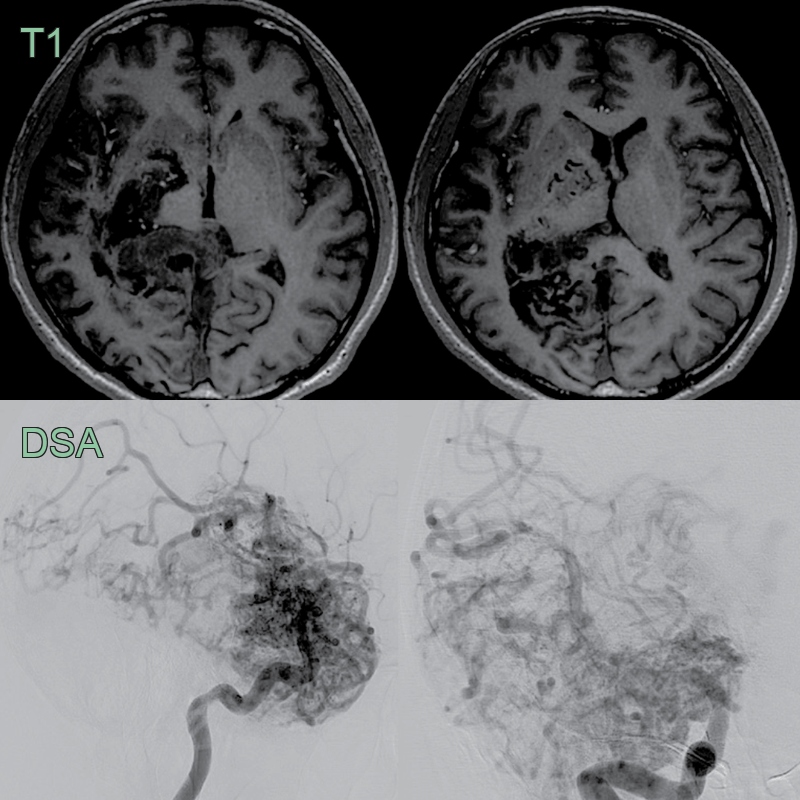
- 20 year old paitent presented with headaches.
- Angiography showed an ill-defined nidus in the right cerebral hemisphere supplied by the anterior circulation.
- Imaging modified from Shomura et al1.
Treatment¶
- Conservative management preferred due to diffuse nature of lesion
- Medical management:
- Antiepileptic drugs for seizure control
- Analgesics for headache management
- Surgical intervention generally not recommended due to high risk
- Targeted endovascular embolisation for specific symptoms:
- Focal seizures
- Progressive neurological deficits
- Stereotactic radiosurgery:
- Limited role due to diffuse nature of lesion
- May be considered for small, focal areas of abnormality
- Regular follow-up and monitoring:
- Clinical assessment
- Neuroimaging to evaluate progression
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Arteriovenous Malformation (AVM) | CPA lacks a dominant feeding artery or nidus; diffuse vascular network |
| Moyamoya Disease | CPA does not show typical "puff of smoke" appearance; lacks progressive stenosis of internal carotid arteries |
| Sturge-Weber Syndrome | CPA lacks facial port-wine stain and leptomeningeal angiomatosis |
| Hereditary Haemorrhagic Telangiectasia | CPA does not show multiple small AVMs or telangiectasias in other organs |
| Cerebral Cavernous Malformation | CPA shows flow voids on MRI, unlike the "popcorn" appearance of cavernomas |
| Dural Arteriovenous Fistula | CPA lacks direct arteriovenous shunting and venous hypertension |
| Capillary Telangiectasia | CPA has more extensive vascular network and larger affected area |
| Glioma with Vascular Proliferation | CPA lacks solid tumour component and infiltrative growth pattern |
| Vein of Galen Malformation | CPA does not involve the deep venous system or show aneurysmal dilatation of the vein of Galen |
| Sinus Pericranii | CPA is intraparenchymal, while sinus pericranii is extracranial |
-
Shomura et al. Multiple Endovascular Treatments for Haemorrhagic Cerebral Proliferative Angiopathy: A Case Report. 2022. Case Reports in Neurology - Open in new tab. ↩