Chiari I malformation¶
Summary

- Congenital hindbrain anomaly characterised by caudal displacement of cerebellar tonsils through foramen magnum
- Presents with headaches, neck pain, and neurological symptoms
- Diagnosed on MRI; treatment ranges from conservative management to surgical decompression
Pathophysiology¶
- Underdevelopment of posterior fossa leads to overcrowding and herniation of cerebellar tonsils
- Obstruction of CSF flow at craniocervical junction
- Associated with syringomyelia in 23-76% of cases
- May be associated with genetic factors or skull base abnormalities
Demographics¶
- Prevalence estimated at 0.1-0.5% of general population
- More common in females (1.3:1 female-to-male ratio)
- Often diagnosed in adolescence or early adulthood
- Can be asymptomatic and discovered incidentally
Diagnosis¶
- Clinical presentation:
- Occipital headaches exacerbated by Valsalva manoeuvre
- Neck pain
- Sensory disturbances
- Balance problems
- Visual symptoms
- Neurological examination may reveal:
- Nystagmus
- Dysarthria
- Lower cranial nerve deficits
- Sensory loss in upper limbs
Imaging¶
- MRI is the gold standard for diagnosis
- Sagittal T1 and T2-weighted sequences of brain and cervical spine
- Key finding: Cerebellar tonsillar herniation ≥5 mm below foramen magnum
- Additional MRI findings:
- Syringomyelia
- Hydrocephalus
- Basilar invagination
- Cine MRI:
- Demonstrates altered CSF flow dynamics at craniocervical junction
- CT:
- May show bony abnormalities of skull base
- Not routinely used for primary diagnosis
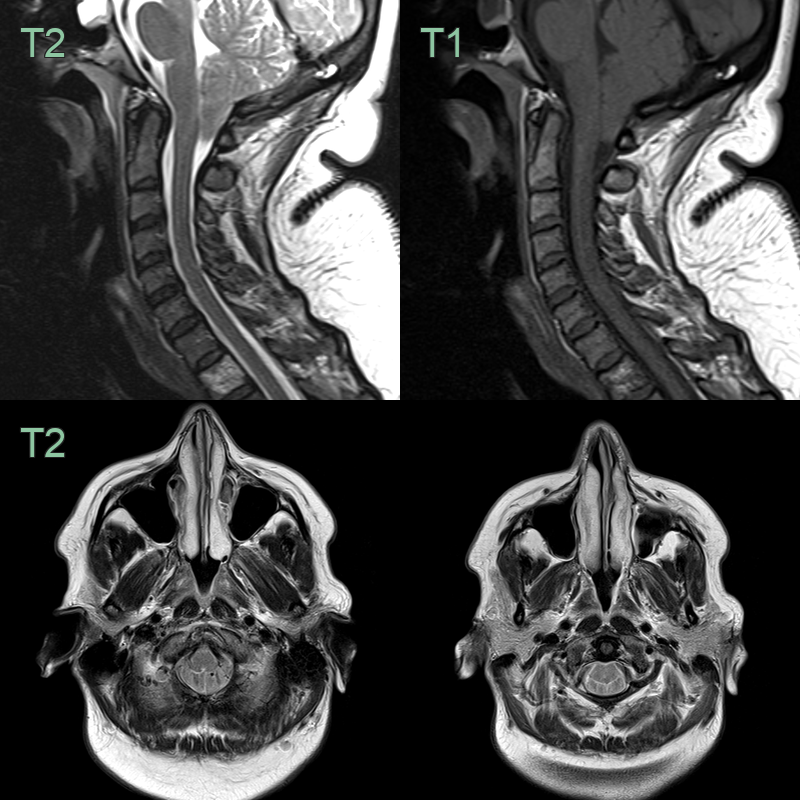
- 40-year-old patient with a cough-induced headache.
- A constitutionally small posterior fossa and low lying tonsils cause crowding of the foramen magnum.
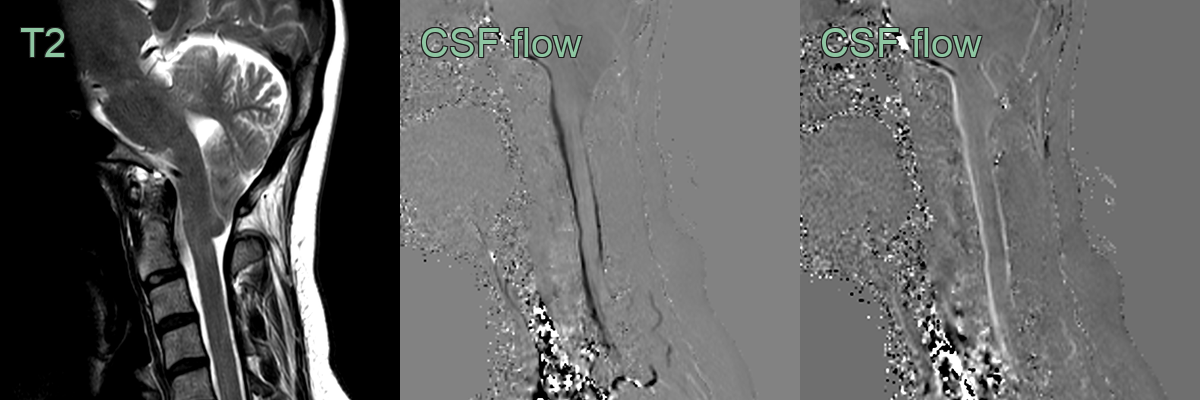
- A 30-year-old patient had an incidental Chiari I malformation.
- The cerebellar tonsils were elongated, sitting 1.2 cm below the foramen magnum causing crowding of the foramen magnum.
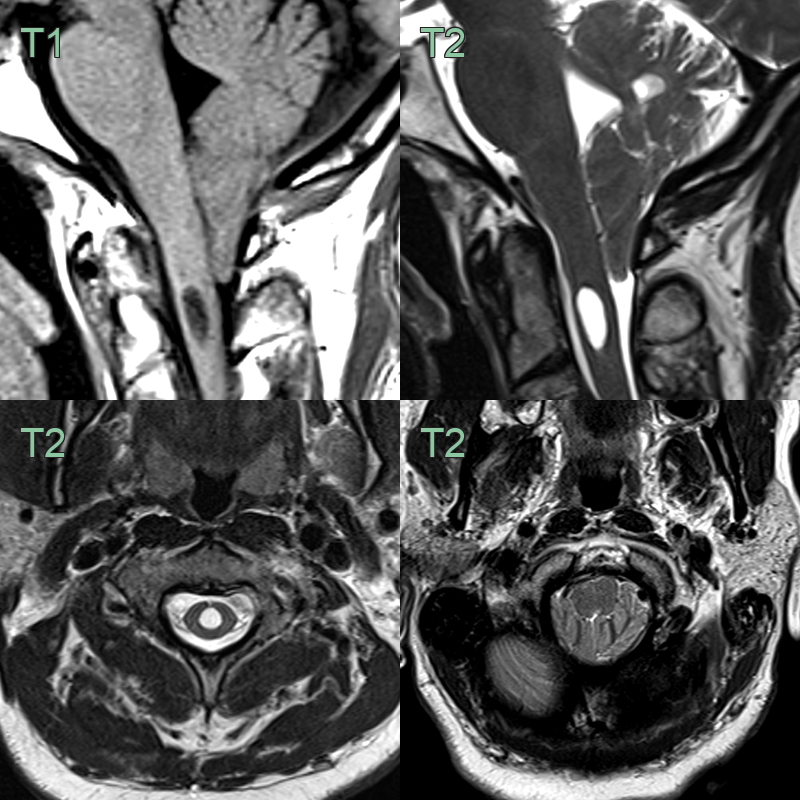
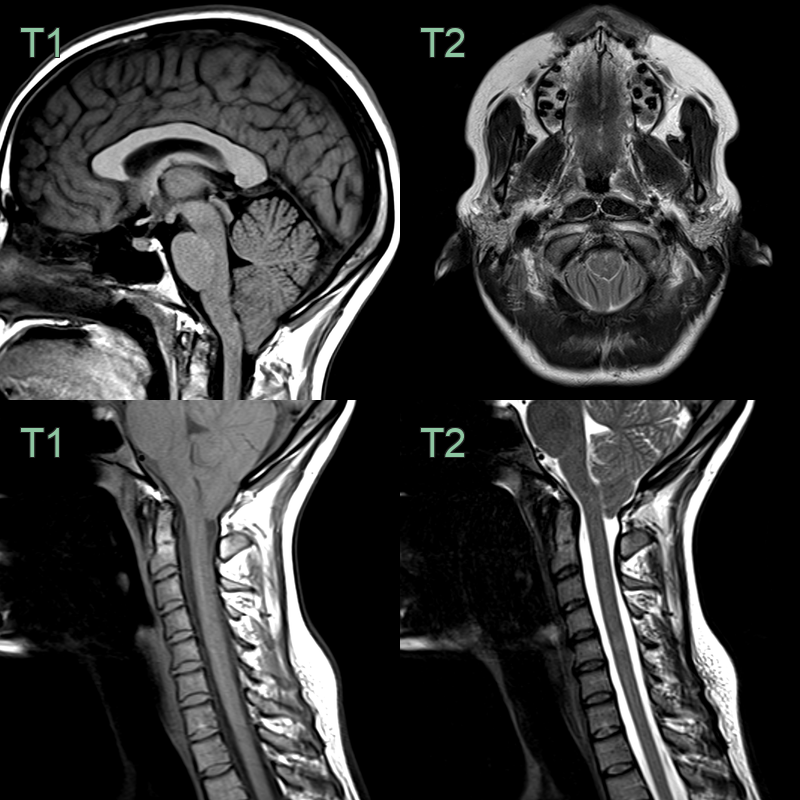
- A 30-year-old patient present with a headache.
- MRI showed peg-like tonsils extending inferiorly behind the cervicomedullary junction and a C2 syrinx.
Treatment¶
- Asymptomatic patients: Observation and follow-up
- Conservative management for mild symptoms:
- Pain management
- Physical therapy
- Lifestyle modifications
- Surgical intervention for severe or progressive symptoms:
- Posterior fossa decompression
- Duraplasty
- C1 laminectomy
- Postoperative imaging:
- MRI to assess adequacy of decompression and resolution of syringomyelia
- Long-term follow-up:
- Monitor for symptom recurrence and complications
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Intracranial hypotension | Orthostatic headaches; MRI shows pachymeningeal enhancement and sagging of brain |
| Syringomyelia | Often coexists with Chiari I, but can occur independently; MRI shows fluid-filled cavity within spinal cord |
| Posterior fossa tumour | MRI shows space-occupying lesion; may have associated hydrocephalus |
| Basilar invagination | Radiographic evidence of odontoid process projecting above foramen magnum; often associated with skeletal dysplasias |
| Dandy-Walker malformation | MRI shows cystic dilatation of 4th ventricle and hypoplasia of cerebellar vermis |