Cholesteatoma¶
Summary
- Cholesteatoma is a benign but locally destructive lesion of the temporal bone, characterised by an accumulation of keratinizing squamous epithelium
- It typically presents with chronic otorrhea, hearing loss, and potential complications due to erosion of surrounding structures
- Imaging plays a crucial role in diagnosis, surgical planning, and follow-up
Pathophysiology¶
- Two main types:
- Congenital: Remnant of embryonic epithelial tissue in the middle ear
- Acquired: Most common, develops from retraction pocket in pars flaccida of tympanic membrane
- Growth occurs through accumulation of desquamated keratin and debris
- Expansion leads to bone erosion through pressure necrosis and enzymatic activity
Demographics¶
- Incidence: 3 per 100,000 in children, 9.2 per 100,000 in adults
- Slightly more common in males
- Peak incidence in second and third decades of life
- Risk factors:
- Chronic otitis media
- Eustachian tube dysfunction
- Craniofacial abnormalities (e.g., cleft palate)
Diagnosis¶
- Clinical presentation:
- Chronic otorrhea
- Progressive conductive hearing loss
- Otalgia
- Vertigo (in advanced cases)
- Otoscopic examination:
- Retraction pocket or attic perforation
- White or pearly mass behind tympanic membrane
- Audiometry:
- Conductive hearing loss
- Sensorineural component in advanced cases
Imaging¶
- CT (non-contrast):
- Modality of choice for initial evaluation and surgical planning
- Findings:
- Soft tissue mass in middle ear or mastoid
- Bone erosion (scutum, ossicles, tegmen tympani)
- Widening of aditus ad antrum
- Labyrinthine fistula (in advanced cases)
- MRI:
- Complementary to CT, especially for follow-up and recurrence detection
- Findings:
- T1: Intermediate to low signal intensity
- T2: Heterogeneous, predominantly high signal intensity
- Diffusion-weighted imaging (DWI): Restricted diffusion, high signal on b1000 images
- Non-echo planar diffusion-weighted imaging (non-EPI DWI):
- Higher sensitivity for small cholesteatomas and recurrence detection
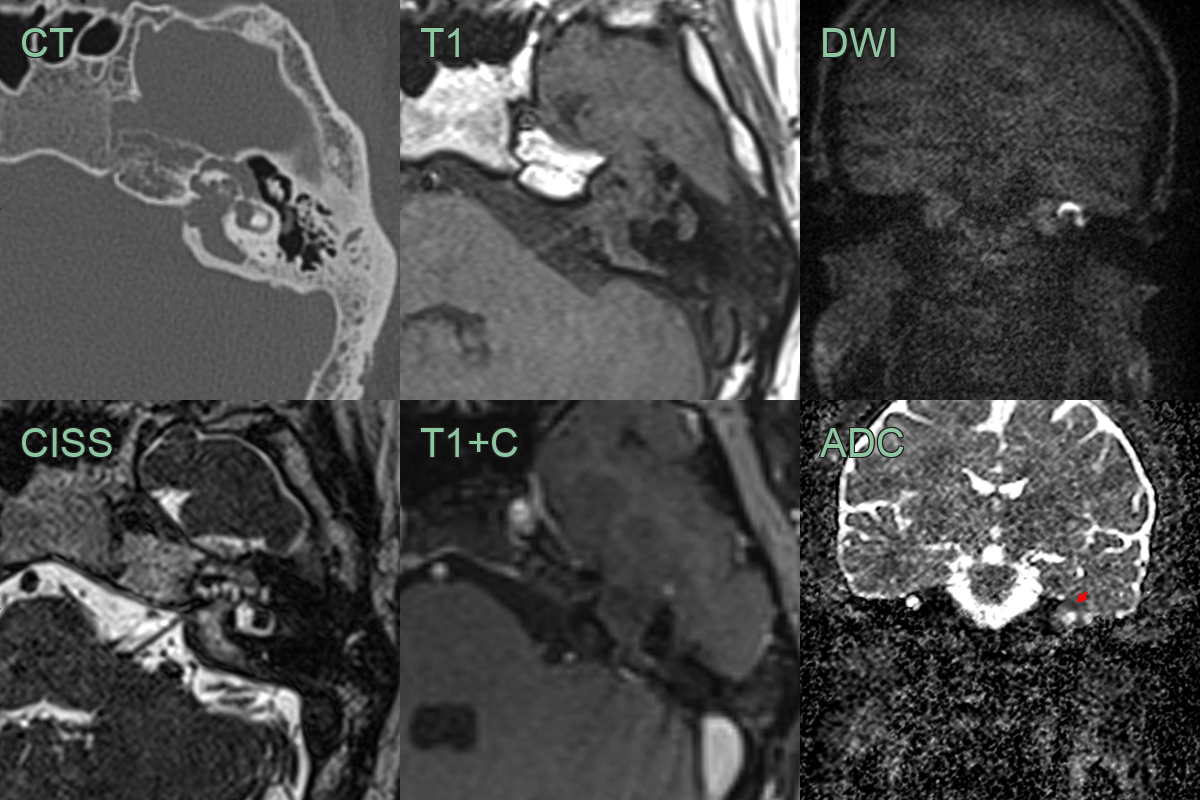
- A 20-year-old patient presented with a facial nerve palsy and sensorineural hearing loss.
- CT showed erosion of the petrous bone including the posterior wall of the internal auditory canal and the wall of the labyrinthine and tympanic facial canal.
- MRI showed a non-enhancingm and T2-hyperintense lesion causing diffusion restriction.
Treatment¶
- Surgical management is the mainstay of treatment
- Surgical approaches:
- Canal wall up (CWU) tympanomastoidectomy
- Canal wall down (CWD) tympanomastoidectomy
- Choice of approach depends on extent of disease and surgeon preference
- Goals of surgery:
- Complete removal of cholesteatoma
- Preservation or reconstruction of hearing mechanism
- Prevention of recurrence
- Postoperative follow-up:
- Regular otoscopic examinations
- Audiometry
- Imaging (CT or MRI) to detect recurrence
- Complications if left untreated:
- Intracranial extension
- Facial nerve paralysis
- Labyrinthine fistula
- Meningitis
- Brain abscess
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Chronic otitis media | Lack of keratin debris on imaging |
| Epidermoid cyst | Markedly restricted diffusion; typically occurs in CPA cistern or other extra-otologic sites |
| Paraganglioma | Characteristic "salt and pepper" appearance on MRI |
| Cholesterol granuloma | Hyperintense on T1-weighted MRI |
| Langerhans cell histiocytosis | Typically multifocal lesions |