Cholesterol Granuloma¶
Summary
- Cholesterol granuloma is a benign, expansile cystic lesion containing cholesterol crystals, haemosiderin, and fibrous tissue
- Typically occurs in the temporal bone, particularly the petrous apex
- Imaging shows a well-defined, expansile lesion with characteristic MRI signal intensities
Pathophysiology¶
- Believed to result from a foreign body reaction to cholesterol crystals
- Proposed mechanisms:
- Obstruction of pneumatised air cells leading to haemorrhage and inflammation
- Chronic haemorrhage into a confined space (e.g., mucosal retention cyst)
- Cholesterol crystals form from degraded blood products
- Surrounding granulation tissue develops, leading to expansion and bone remodelling
Demographics¶
- Can occur at any age, but most common in adults
- Slight male predominance (male:female ratio approximately 1.5:1)
- No known racial predilection
Diagnosis¶
- Often asymptomatic and discovered incidentally
- When symptomatic, presentation depends on location:
- Petrous apex: hearing loss, tinnitus, vertigo, facial nerve palsy
- Orbit: proptosis, diplopia, visual disturbances
- Paranasal sinuses: nasal obstruction, facial pain
- Differential diagnosis includes:
- Cholesteatoma
- Mucocele
- Arachnoid cyst
- Epidermoid cyst
Imaging¶
- CT findings:
- Well-defined, expansile lesion with smooth margins
- Bone remodelling without destruction
- Variable density, often isodense to brain
- May show fluid-fluid levels
- MRI findings :
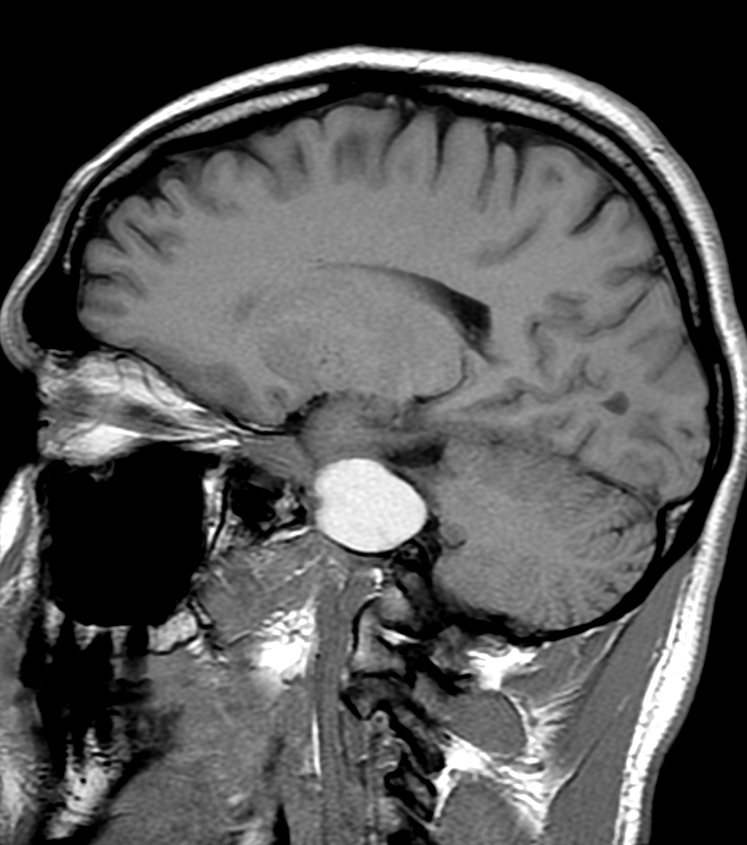
- T1-weighted: Hyperintense due to protein content and methaemoglobin
- T2-weighted: Heterogeneous, often hyperintense
- Gradient echo: Susceptibility artefact due to haemosiderin
- Post-contrast: Thin peripheral enhancement
- Characteristic "motor oil" appearance on MRI due to T1 hyperintensity and T2 heterogeneity
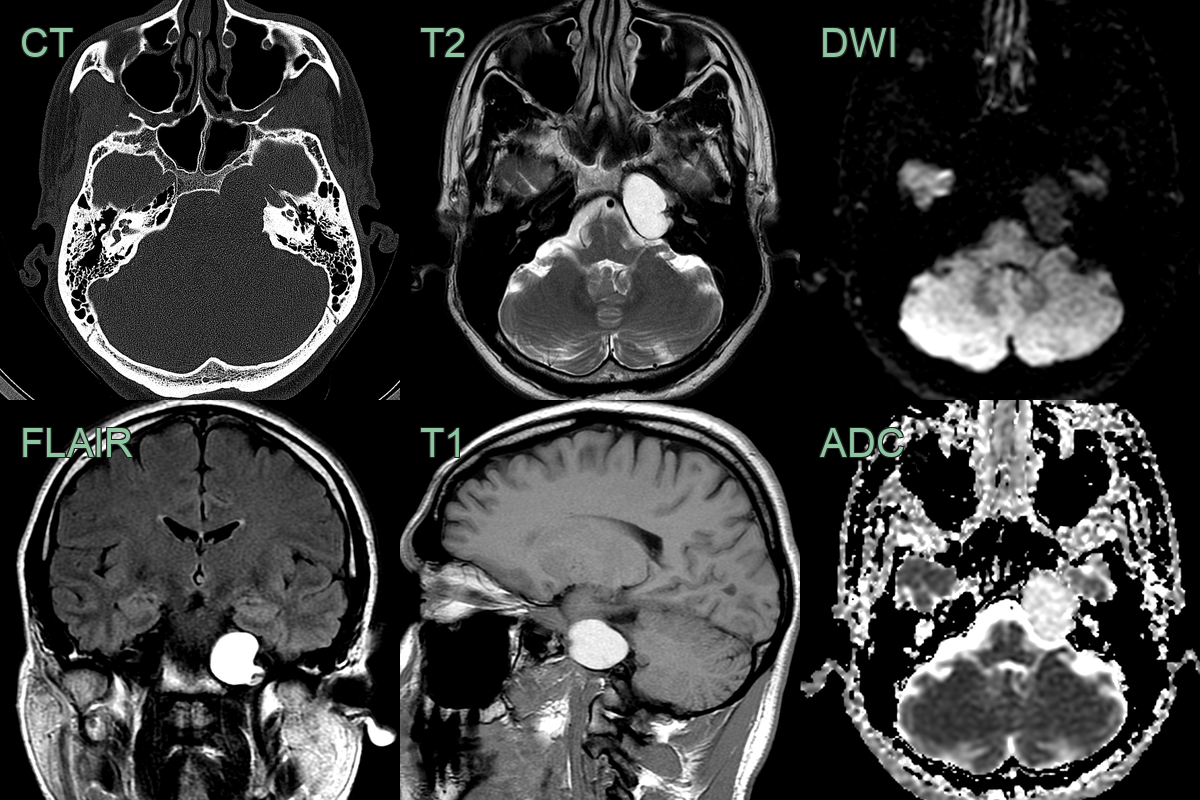
- A 50 year old presented with a headache.
- CT showed a well-marginated lesion in the left petrous apex.
- T1-hyperintensity within the lesion was consitent with a cholesterol granuloma.
- Following enlargement and worsening headaches, the lesion was drained (not shown).
Treatment¶
- Asymptomatic lesions: Observation with serial imaging
- Symptomatic lesions:
- Surgical drainage and marsupialization
- Endoscopic approaches preferred when feasible
- Complete removal of capsule not necessary
- Stereotactic radiation therapy: Alternative for surgically challenging locations
- Recurrence is uncommon but can occur, necessitating long-term follow-up
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cholesteatoma | Lacks characteristic "popcorn" appearance on T2-weighted MRI |
| Acoustic neuroma | Typically arises from internal auditory canal, not petrous apex |
| Meningioma | Usually enhances strongly with contrast on MRI |
| Arachnoid cyst | Follows CSF signal on all MRI sequences |
| Epidermoid cyst | Restricted diffusion on DWI |
| Mucocele | Lacks T1 hyperintensity characteristic of cholesterol granuloma |
| Petrous apex effusion | Lacks expansile nature and chronic symptoms |
| Metastasis | Often multiple lesions; bone destruction with irregular margins |