Chondrosarcoma¶
Summary
- Malignant cartilaginous tumour arising from bone or soft tissue
- Characterised by production of cartilage matrix
- Imaging shows lobulated, lytic lesion with ring and arc calcifications
Pathophysiology¶
- Arises from cartilage-forming cells or mesenchymal stem cells
- Classified into three grades based on cellularity, nuclear atypia, and mitotic activity
- Subtypes include conventional, clear cell, dedifferentiated, and mesenchymal chondrosarcoma
Demographics¶
- Second most common primary bone tumour after osteosarcoma
- Peak incidence in 5th to 7th decades of life
- Slight male predominance (1.5:1)
- Most common sites: pelvis, proximal femur, proximal humerus, and ribs
Diagnosis¶
- Clinical presentation:
- Pain and swelling at the affected site
- Pathological fracture in advanced cases
- Histopathology:
- Lobulated architecture with hyaline cartilage matrix
- Varying degrees of cellularity and nuclear atypia
- Molecular markers:
- IDH½ mutations in conventional and dedifferentiated subtypes
Imaging¶
- Plain radiographs:
- Lytic lesion with endosteal scalloping and cortical thickening
- Punctate or ring-and-arc calcifications
- CT:
- Better delineation of calcifications and cortical involvement
- Useful for staging and surgical planning
- MRI:
- T1: low to intermediate signal intensity
- T2: high signal intensity with lobulated appearance
- Enhancement pattern varies with grade
- Bone scintigraphy:
- Increased uptake, useful for detecting metastases
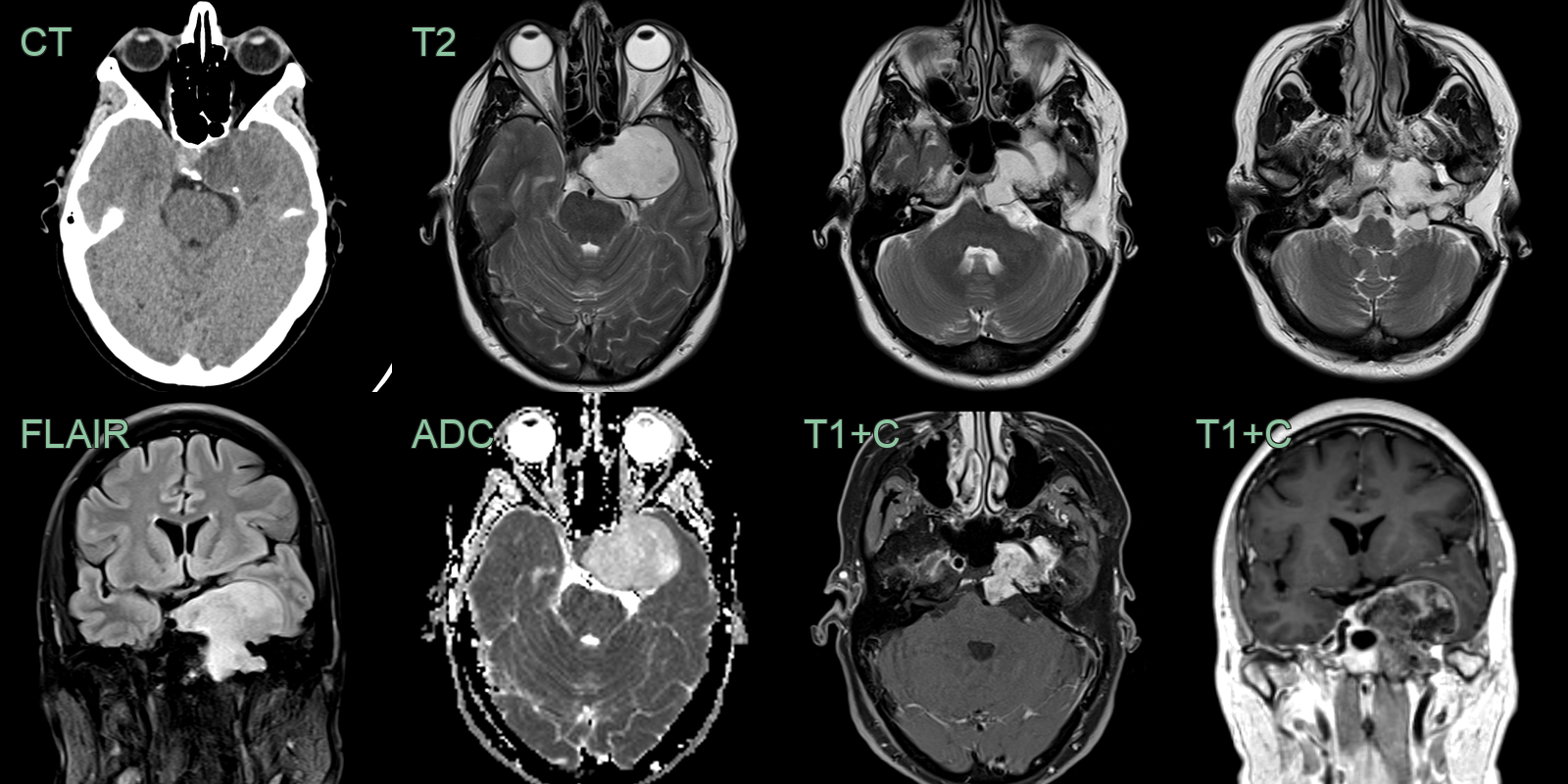
- A 50 year old patient presented with diplopia.
- Imaging showed a large enhancing non-calcified lesion centred on the left petrous apex with invasion of the cavernous sinus.
Treatment¶
- Surgical resection is the mainstay of treatment
- Wide surgical margins are crucial for local control
- Chemotherapy:
- Limited efficacy in conventional chondrosarcoma
- May be beneficial in mesenchymal and dedifferentiated subtypes
- Radiation therapy:
- Adjuvant treatment for positive margins or high-grade tumours
- Primary treatment for inoperable cases
- Targeted therapies:
- IDH inhibitors under investigation for IDH-mutant chondrosarcomas
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Enchondroma | Lack of endosteal scalloping and cortical destruction |
| Osteosarcoma | Presence of osteoid matrix; more aggressive appearance |
| Giant Cell Tumour | Epiphyseal location; lack of chondroid matrix |
| Fibrous Dysplasia | Ground-glass appearance; lack of cartilaginous matrix |
| Metastatic Disease | Multiple lesions; no chondroid matrix; destructive without expansile remodelling |
| Chondroblastoma | Typically in epiphysis of long bones; smaller size; calcified matrix; marked surrounding oedema |
| Aneurysmal Bone Cyst | Fluid-fluid levels on MRI; expansile thin cortical shell; no mineralised chondroid matrix |
| Ewing Sarcoma | Onion-skin or sunburst periosteal reaction; permeative pattern; soft tissue mass; no chondroid matrix |
| Chondromyxoid Fibroma | Eccentric location; lobulated appearance |
| Osteochondroma | Surface lesion with cartilage cap; no medullary involvement |