Choroid Plexus Xanthogranuloma¶
Summary
- Rare, benign intracranial lesion arising from the choroid plexus
- Characterised by accumulation of lipid-laden macrophages (xanthoma cells)
- Typically asymptomatic and incidentally discovered on imaging or autopsy
Pathophysiology¶
- Exact etiology remains unclear
- Hypothesized mechanisms:
- Chronic inflammation of choroid plexus epithelium
- Accumulation of lipids due to breakdown of red blood cells
- Possible association with metabolic disorders or hyperlipidaemia
- Histologically characterised by:
- Foamy macrophages (xanthoma cells)
- Cholesterol clefts
- Haemosiderin deposits
- Multinucleated giant cells
Demographics¶
- Rare condition, true incidence unknown
- More commonly found in adults, particularly in the elderly
- No significant gender predilection reported
- Increased prevalence in autopsy studies (up to 1.6-7% of cases)
Diagnosis¶
- Often asymptomatic and discovered incidentally
- When symptomatic, may present with:
- Headaches
- Dizziness
- Cognitive decline
- Focal neurological deficits (rare)
- Definitive diagnosis requires histopathological examination
Imaging¶
- CT findings:
- Hyperdense lesion within the choroid plexus
- May show calcifications
- MRI findings:
- T1-weighted: Hyperintense due to lipid content
- T2-weighted: Variable signal intensity
- Gradient echo: May show susceptibility artefacts due to haemosiderin
- Contrast enhancement: Typically minimal to none
- Differential diagnosis:
- Choroid plexus papilloma
- Meningioma
- Metastasis
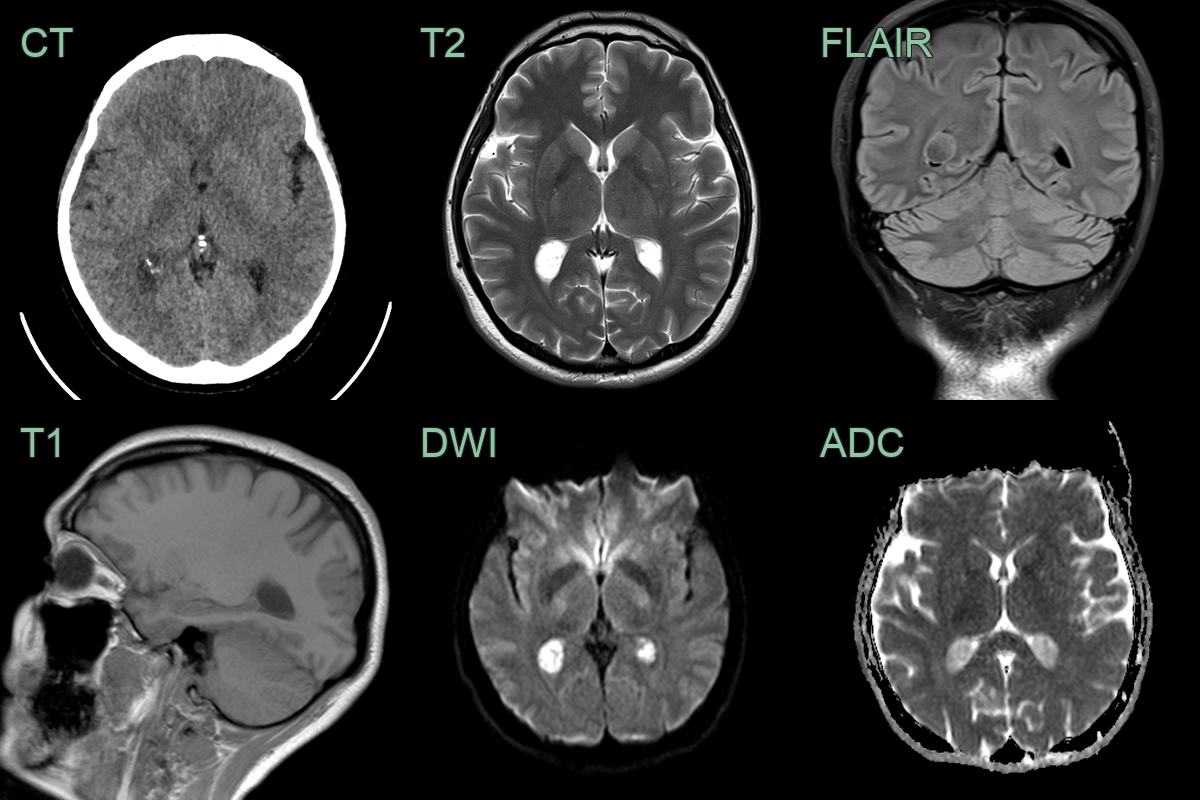
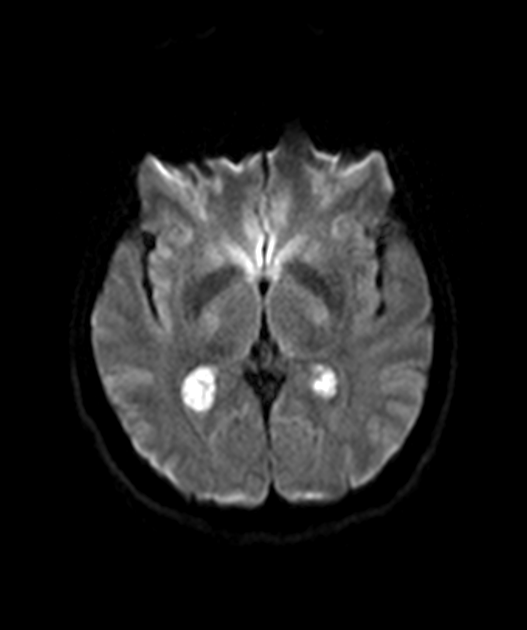
- The choroid plexus within the trigones of the lateral ventricles were expanded and hyperintense on diffusion-weighted imaging.
Treatment¶
- Asymptomatic lesions:
- Conservative management with regular imaging follow-up
- Symptomatic lesions:
- Surgical resection may be considered
- Complete resection generally curative
- Post-treatment follow-up:
- Regular imaging to monitor for recurrence
- No standardized follow-up protocol due to rarity of the condition
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Choroid plexus papilloma | Lacks calcification; typically enhances more homogeneously |
| Meningioma | Usually extra-ventricular; dural tail sign may be present |
| Ependymoma | More heterogeneous appearance; may have cystic components |
| Metastasis | Multiple lesions; irregular enhancement; surrounding oedema; no fat or calcium signal |
| Choroid plexus carcinoma | More aggressive appearance; invasion of surrounding tissue |
| Intraventricular haemorrhage | Acute onset; fluid-fluid levels on imaging |
| Subependymoma | Typically in lateral ventricle angles; less enhancement |
| Central neurocytoma | Usually attached to septum pellucidum; calcifications common |
| Intraventricular tuberculoma | Concomitant basal meningitis; ring enhancement |