Creutzfeldt-Jakob disease (CJD)
Summary
- Rare, fatal neurodegenerative disorder characterised by rapidly progressive dementia
- Caused by abnormal prion protein accumulation in the brain
- Imaging findings include cortical ribboning and basal ganglia hyperintensities on DWI/FLAIR
Pathophysiology
- Accumulation of abnormally folded prion proteins (PrPSc) in the brain
- Leads to neuronal loss, gliosis, and spongiform changes
- Four subtypes:
- Sporadic (sCJD): Most common (85-90% of cases)
- Familial (fCJD): Genetic mutations in PRNP gene
- Iatrogenic (iCJD): Transmission via contaminated medical procedures
- Variant (vCJD): Linked to bovine spongiform encephalopathy (BSE)
Demographics
- Incidence: 1-2 cases per million population per year
- Median age of onset:
- sCJD: 60-65 years
- vCJD: 26-28 years
- No gender predilection
- Geographical distribution: Worldwide, with higher incidence in some countries due to genetic factors
Diagnosis
- Clinical presentation:
- Rapidly progressive dementia
- Myoclonus
- Visual disturbances
- Cerebellar ataxia
- Diagnostic criteria:
- WHO criteria for probable CJD
- MRI findings
- CSF biomarkers (14-3-3 protein, tau protein, RT-QuIC)
- EEG: Periodic sharp wave complexes
- Definitive diagnosis: Brain biopsy or post-mortem examination
Imaging
- MRI:
- DWI/FLAIR:
- Cortical ribboning (high signal in cortical grey matter)
- Basal ganglia hyperintensities (caudate and putamen)
- Thalamic hyperintensities (pulvinar sign in vCJD)
- T2-weighted:
- Subtle hyperintensities in affected areas
- CT:
- Generally normal in early stages
- May show cerebral atrophy in advanced cases
- PET:
- Hypometabolism in affected cortical regions and basal ganglia
- SPECT:
- Reduced perfusion in affected areas
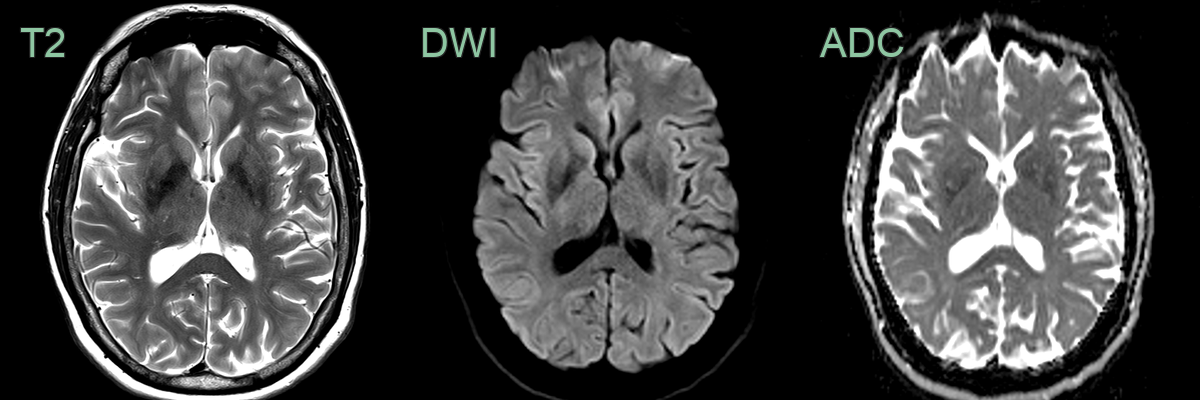
- 65-year-old male presented with myoclonus and cogntive impairement.
- On the inital MRI, rather equivocal DWI hyperintensity in the corpora striatum became obvious 6 months later.
- A 71-year-old female developed progressively worsening confusion and visual hallucinations.
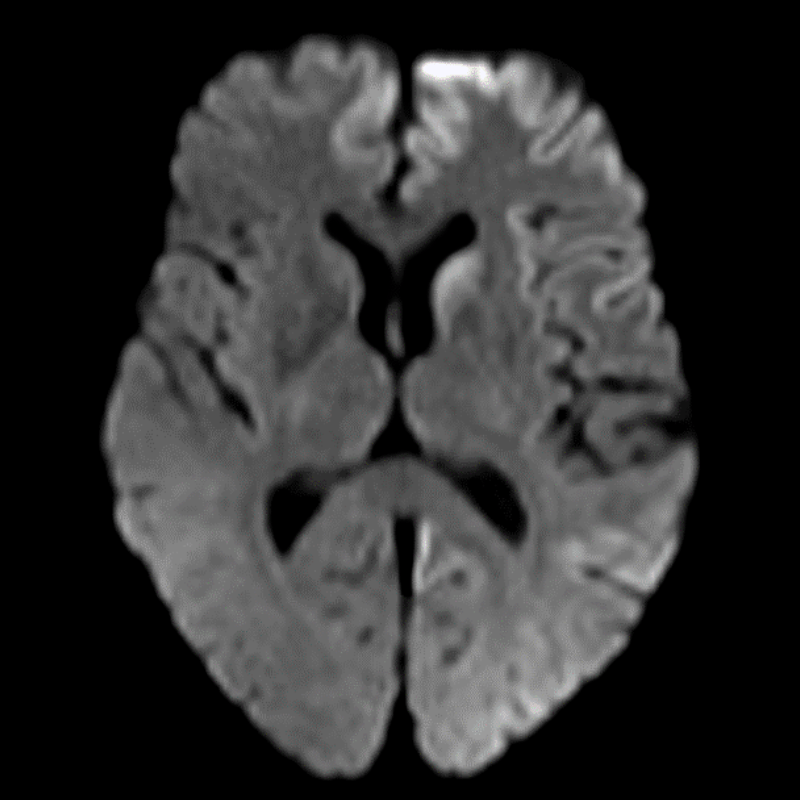
- Cortical ribboning on DWI was most apparent in the left caudate head, frontal lobe and parietal lobe.
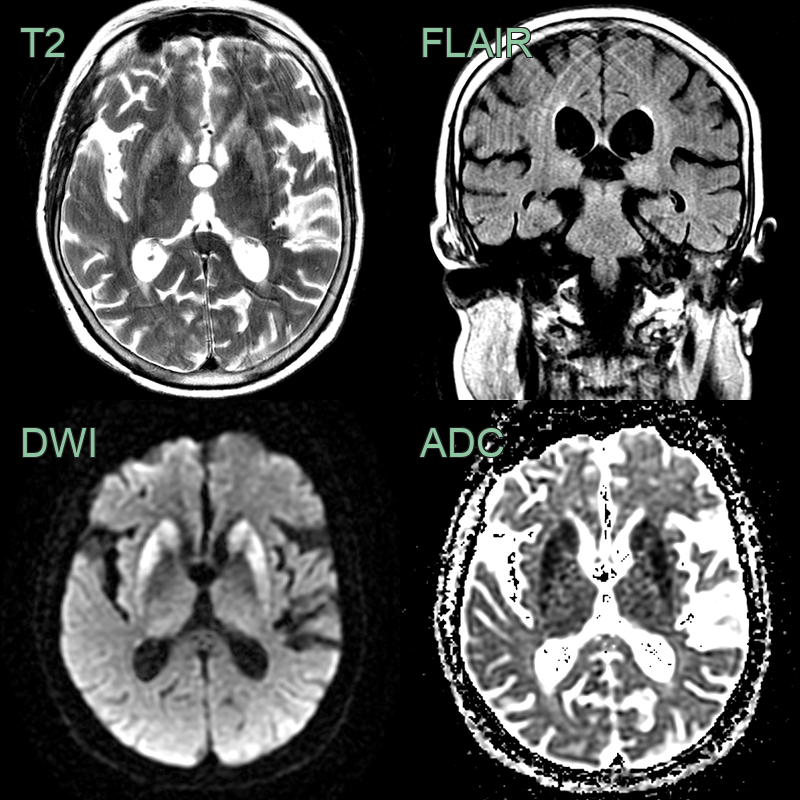
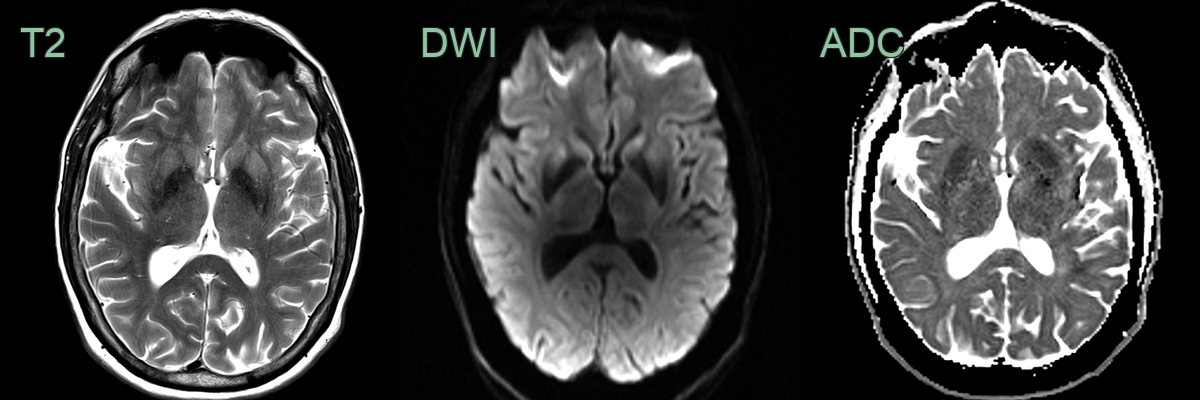
- A 65-year-old patient presented with rapidly progressive cogntive impairment and cerebellar ataxia.
- There was diffusion restriction in the striatum and FLAIR hyperintensity, without diffusion restriction, in the pulvinar of the thalami.
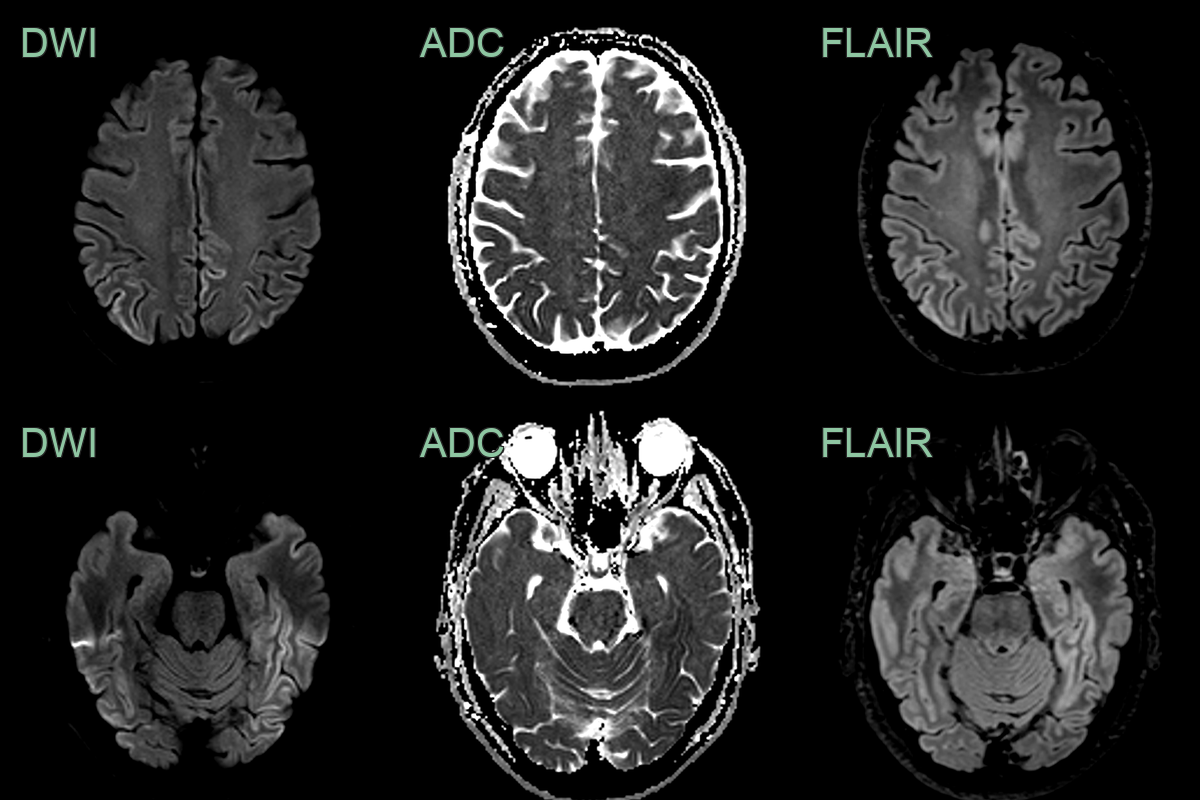
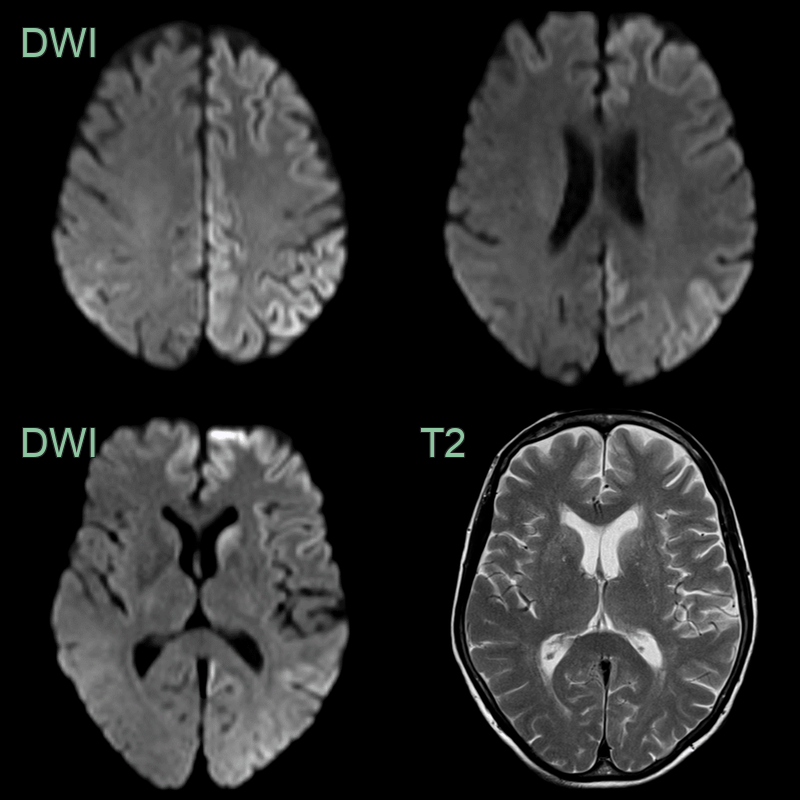
- Patient with recent onset cognitive impairment.
- MRI showed assymetrical extensive cortical ribboning in the parietal, occipital and temporal lobes.
Treatment
- No curative treatment available
- Management focuses on supportive care and symptom control:
- Antiepileptic drugs for myoclonus
- Anxiolytics and antidepressants for behavioural symptoms
- Nutritional support
- Experimental therapies:
- Quinacrine: Antiprion activity in vitro, but no proven efficacy in clinical trials
- Doxycycline: Failed to show significant benefit in randomised controlled trial
- Prevention:
- Strict infection control measures in healthcare settings
- Surveillance and control of BSE in cattle
- Genetic counselling for familial cases
Differential diagnosis
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Paraneoplastic/autoimmune limbic encephalitis | Bilateral mesial temporal FLAIR hyperintensity without cortical ribboning; may enhance |
| Viral encephalitis (HSV) | Asymmetric mesial temporal/insular haemorrhagic FLAIR hyperintensity without cortical ribboning |
| Wernicke's encephalopathy | Symmetric T2 hyperintensity of mammillary bodies, periaqueductal grey, and medial thalami |
| Autoimmune encephalitis | Bilateral hippocampal FLAIR hyperintensity; cortical DWI restriction absent |