Clival Metastasis¶
Summary
- Clival metastasis is a rare occurrence of tumour spread to the clivus bone at the skull base
- Typically presents with cranial nerve palsies and headache
- Imaging shows a destructive lesion in the clivus, often with soft tissue extension
Pathophysiology¶
- Hematogenous spread of primary malignancy to the clivus
- Common primary sites include:
- Prostate cancer
- Breast cancer
- Lung cancer
- Thyroid cancer
- Renal cell carcinoma
- Metastatic cells invade and replace normal bone marrow in the clivus
- Local destruction of bone and potential extension into surrounding structures
Demographics¶
- Rare condition, exact incidence unknown
- More common in adults with known primary malignancies
- Slight male predominance reported in some studies
- Peak incidence in 5th to 7th decades of life
Diagnosis¶
- Clinical presentation:
- Headache (most common symptom)
- Cranial nerve palsies (particularly VI, IX, X, XI, XII)
- Diplopia
- Facial numbness or pain
- Dysphagia
- Laboratory tests:
- Elevated tumour markers specific to primary malignancy
- Complete blood count may show anaemia or thrombocytopenia
- Biopsy:
- Often required for definitive diagnosis
- Performed under image guidance (CT or MRI)
Imaging¶
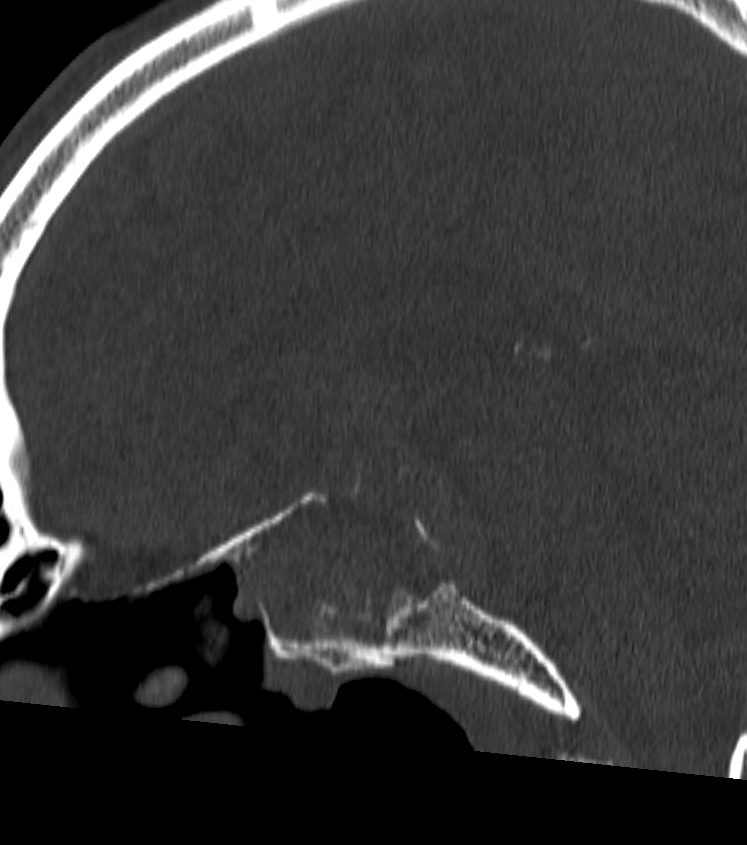
- CT:
- Lytic lesion in the clivus with cortical destruction
- Soft tissue mass may be visible
- Useful for assessing bony involvement and planning biopsy
- MRI:
- T1: Hypointense lesion replacing normal hyperintense bone marrow
- T2: Variable signal intensity
- Post-contrast: Heterogeneous enhancement
- DWI: Often shows restricted diffusion
- Superior for evaluating soft tissue extension and cranial nerve involvement
- Nuclear Medicine:
- PET/CT: Increased FDG uptake in the clival lesion
- Bone scan: Focal increased uptake in the clivus
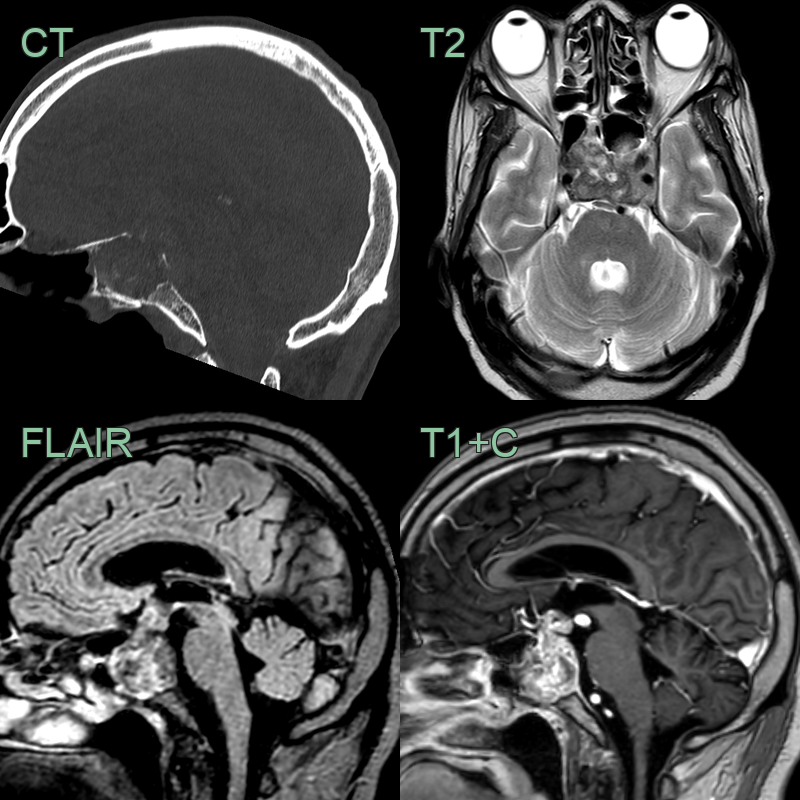
- 55-year-old patient with lung cancer presented with diplopia.
- MRI showed a destructive and enhancing clival lesion that extended into the pituitary fossa and suprasellar space.
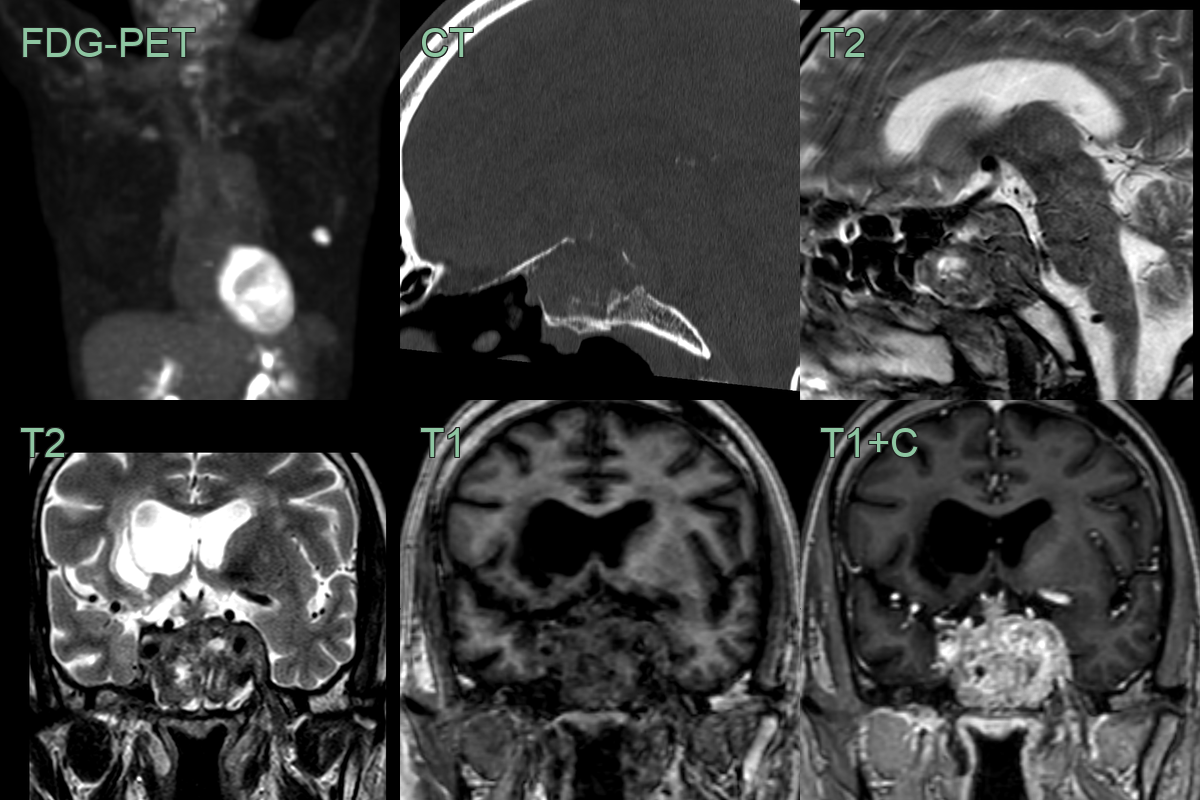
- A 60-year-old patient with a recent lung cancer diagnosis presented wiht headache and diplopia.
- CT showed a destructive lesion in the clivus and pitutiary fossa.
- MRI showed a heterogeneously enhancing lesion invading the left cavernous sinus.
Treatment¶
- Multidisciplinary approach involving oncology, radiation oncology, and neurosurgery
- Treatment options:
- Systemic therapy based on primary malignancy
- Radiation therapy:
- External beam radiation
- Stereotactic radiosurgery for smaller lesions
- Surgery:
- Limited role due to complex anatomy
- May be considered for solitary metastasis or diagnostic biopsy
- Palliative care:
- Pain management
- Supportive care for cranial nerve deficits
- Prognosis:
- Generally poor, as clival metastasis often indicates advanced disease
- Median survival varies depending on primary malignancy and overall disease burden
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Chordoma | Typically midline and expansile; may show characteristic T2 hyperintensity |
| Meningioma | Usually has a dural tail; homogeneous enhancement |
| Pituitary macroadenoma | Centered in sella turcica; may have suprasellar extension |
| Nasopharyngeal carcinoma | Originates from nasopharynx; often with lateral extension |
| Lymphoma | More homogeneous appearance; may have restricted diffusion |
| Plasmacytoma | Typically hyperdense on CT; may have associated bone destruction |
| Chondrosarcoma | Off-midline location; may show characteristic calcifications |
| Osteomyelitis | May show surrounding bone oedema; clinical history of infection |
| Fibrous dysplasia | Ground-glass appearance on CT; typically expands bone |
| Eosinophilic granuloma | Typically occurs in younger patients; may have beveled edge appearance |