Colloid Cyst
Summary
- Benign intracranial cyst typically located in the anterior third ventricle
- Presents with intermittent obstructive hydrocephalus and headaches
- Characteristic appearance on CT and MRI as a round, well-defined lesion
Pathophysiology
- Believed to originate from endodermal elements during embryogenesis
- Composed of a thin collagenous capsule lined by epithelial cells
- Contains viscous, gelatinous fluid rich in mucin and cholesterol crystals
- May cause obstruction of the foramen of Monro, leading to hydrocephalus
Demographics
- Accounts for 0.5-2% of all intracranial tumours
- Most commonly diagnosed in adults aged 20-50 years
- Slight male predominance (1.5:1 male to female ratio)
- Rare in children and elderly
Diagnosis
- Clinical presentation:
- Intermittent headaches (most common symptom)
- Nausea and vomiting
- Visual disturbances
- Memory deficits
- Sudden loss of consciousness (rare, but potentially fatal)
- Physical examination:
- Often normal between symptomatic episodes
- Papilledema may be present in cases of increased intracranial pressure
Imaging
- CT findings:
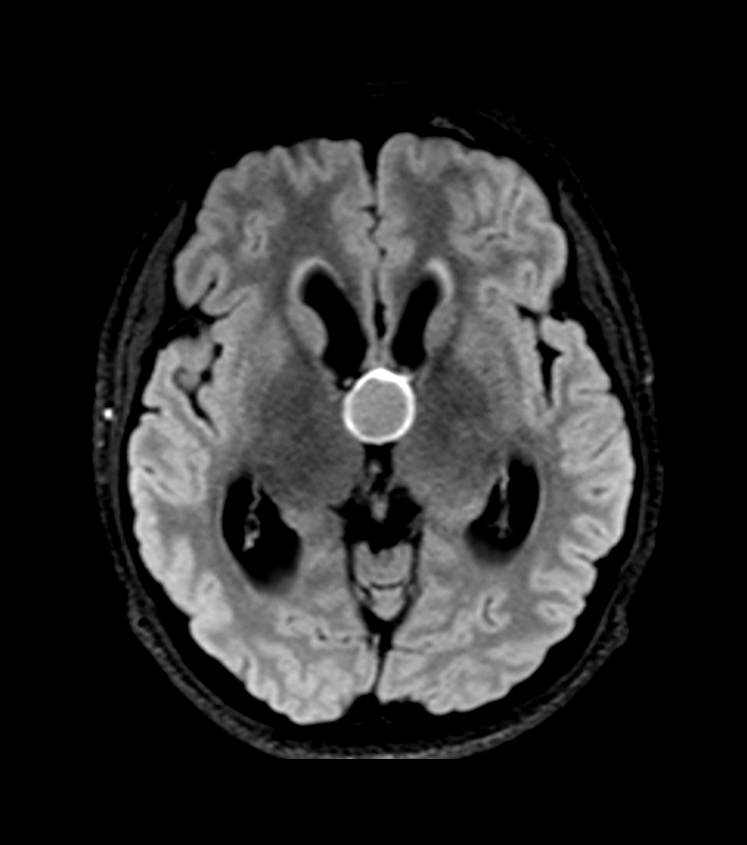
- Hyperdense, round lesion in the anterior third ventricle
- Usually measures 3-15 mm in diameter
- May demonstrate rim calcification
- MRI findings:
- T1-weighted: Variable signal intensity (hyperintense to CSF)
- T2-weighted: Usually hypointense to CSF
- FLAIR: Hyperintense signal
- Contrast enhancement: Typically minimal or absent
- DWI: No restricted diffusion
- Differential diagnosis:
- Subependymoma
- Central neurocytoma
- Choroid plexus papilloma
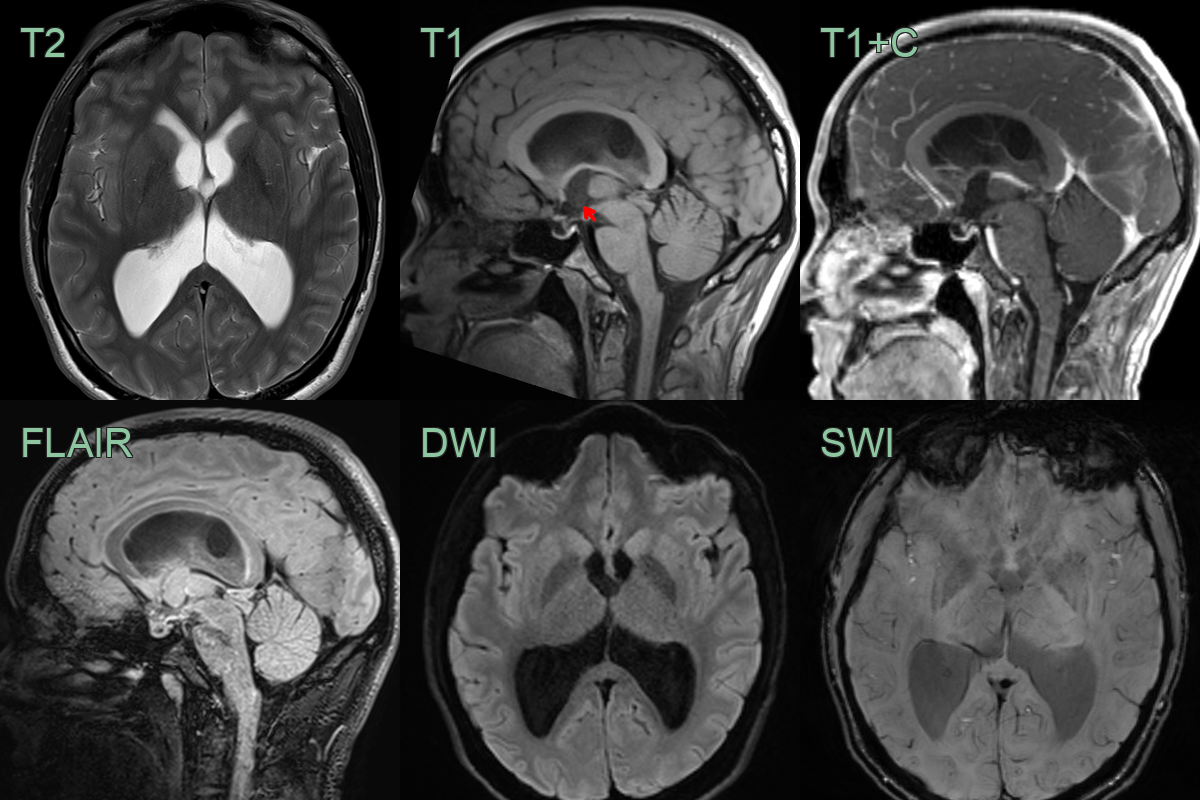
- A well-demarcated T1-hyperinse lesion in the third ventricle at the level of the foramina of Monro.
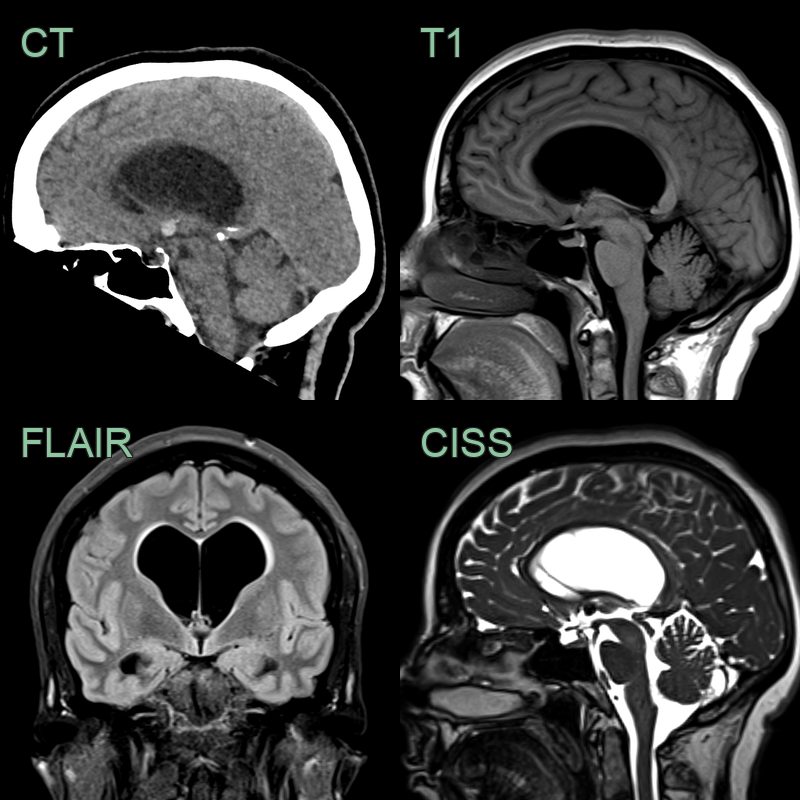
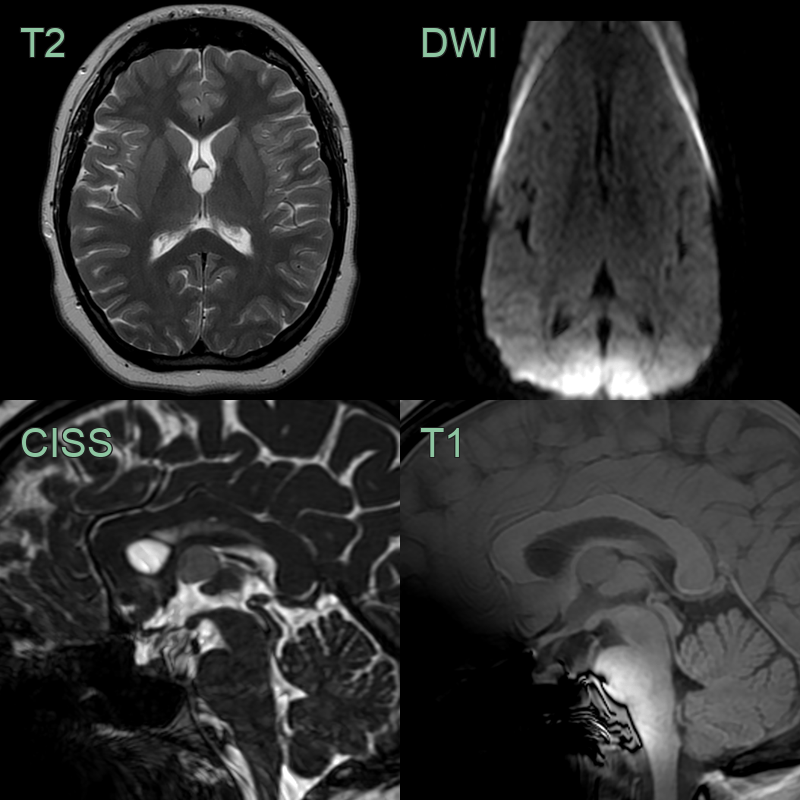
- 55-year-old patient presented with bladder dysfunction and unsteadiness.
- CT showed a 7 mm hyperdense lesion filling the foramen of Monro and marked enlargement of the ventricles.
- There was very little periventricular oedeam, and so the appearances suggest chronic, compensated, ventriculomeagly (rather than acute hydrocephalus).
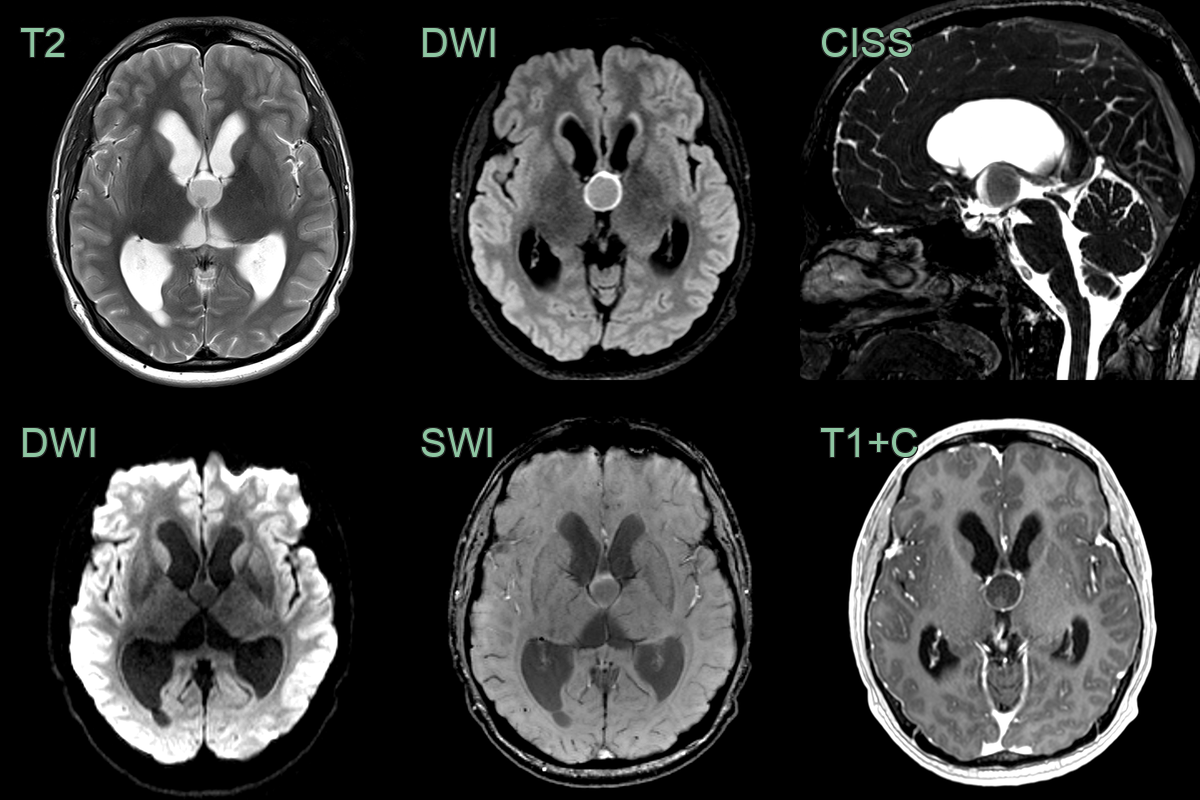
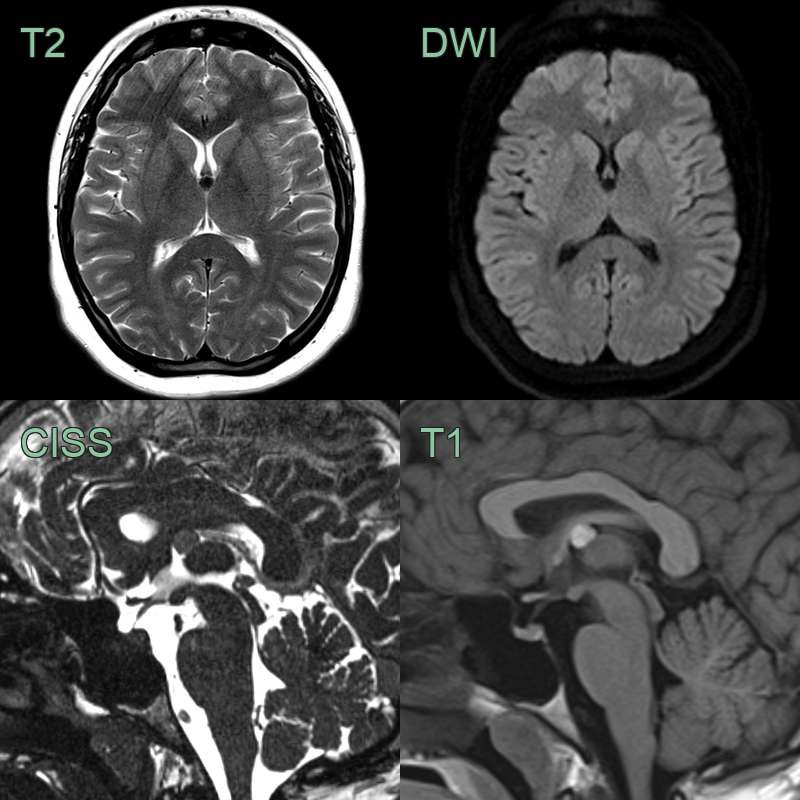
- A 20-year-old patient presented with an acute onset severe headache and reduced GCS.
- MRI showed a non-enhancing cyst near the foramina of Monro and acute hydrocephalus.
Treatment
- Observation:
- For small, asymptomatic cysts
- Regular follow-up imaging recommended
- Surgical options:
- Microsurgical resection: Traditional open craniotomy approach
- Endoscopic resection: Minimally invasive technique with lower complication rates
- Stereotactic aspiration: Less invasive but higher recurrence rates
- Complications:
- Recurrence (more common with incomplete resection)
- Memory deficits
- Hypothalamic dysfunction
- Venous infarction (rare)
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Choroid plexus cyst | Located in lateral ventricles rather than third ventricle |
| Arachnoid cyst | Typically extra-axial and follows CSF signal on all sequences |
| Subependymoma | Usually in fourth ventricle or lateral ventricles |
| Central neurocytoma | Typically attached to septum pellucidum in lateral ventricles |
| Craniopharyngioma | Usually suprasellar with calcifications and cystic components |
| Pituitary macroadenoma | Originates from sella turcica, enhances with contrast |
| Epidermoid cyst | Diffusion restriction on DWI, irregular margins |
| Pineal cyst | Located in pineal region, thin-walled |
| Intraventricular meningioma | Enhances strongly with contrast, often calcified |
| Ependymoma | More common in children, enhances with contrast |