Compressive myelopathy¶
Summary
- Compressive myelopathy is a neurological condition characterised by spinal cord compression
- Causes include degenerative changes, tumours, trauma, and congenital abnormalities
- Imaging plays a crucial role in diagnosis and treatment planning
Pathophysiology¶
- Compression of the spinal cord leads to:
- Mechanical disruption of neural tissue
- Vascular compromise and ischaemia
- Inflammatory responses
- Demyelination and axonal degeneration
- Chronic compression may result in:
- Gliosis
- Cystic cavitation
- Atrophy of the spinal cord
Demographics¶
- Incidence varies depending on the underlying cause
- Cervical spondylotic myelopathy:
- Most common cause in adults over 55 years
- Male predominance (2.7:1)
- Traumatic spinal cord injury:
- Higher incidence in young adults and males
- Bimodal distribution: peaks at 15-29 years and >65 years
Diagnosis¶
- Clinical presentation:
- Gait disturbances
- Sensory changes
- Motor weakness
- Bowel and bladder dysfunction
- Physical examination:
- Hyperreflexia
- Positive Hoffman's sign
- Babinski sign
- Decreased proprioception
- Diagnostic tests:
- Electromyography (EMG)
- Nerve conduction studies
- Somatosensory evoked potentials (SSEPs)
Imaging¶
- Magnetic Resonance Imaging (MRI):
- Gold standard for diagnosis
- T2-weighted images: hyperintense signal within the cord
- T1-weighted images: assess for cord atrophy
- Gadolinium-enhanced T1: evaluate for tumours or infection
- Diffusion Tensor Imaging (DTI): assess white matter tract integrity
- Computed Tomography (CT):
- Useful for assessing bony abnormalities
- CT myelography: alternative when MRI is contraindicated
- Plain radiographs:
- Limited utility but may show:
- Degenerative changes
- Fractures
- Congenital anomalies
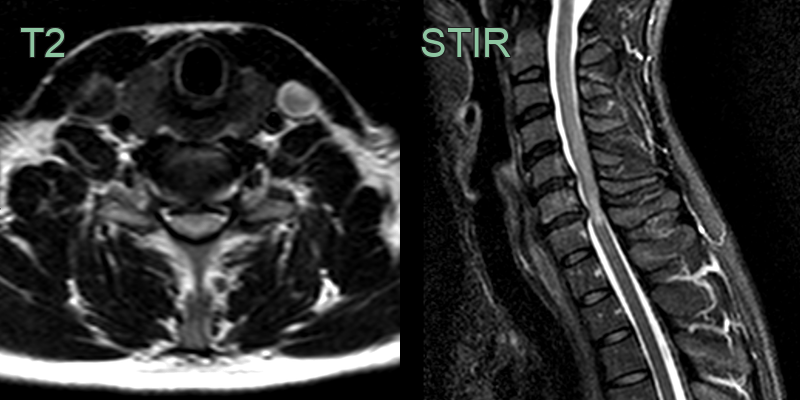
- 70-year-old patient with rheumatoid arthritis presented with tingling in lower limbs and worsening gait.
- There was no significant vertebral canal stenosis but the T2-hyperintense foci in both sides of the cord at C4-5 suggested a chronic compressive myelopathy.

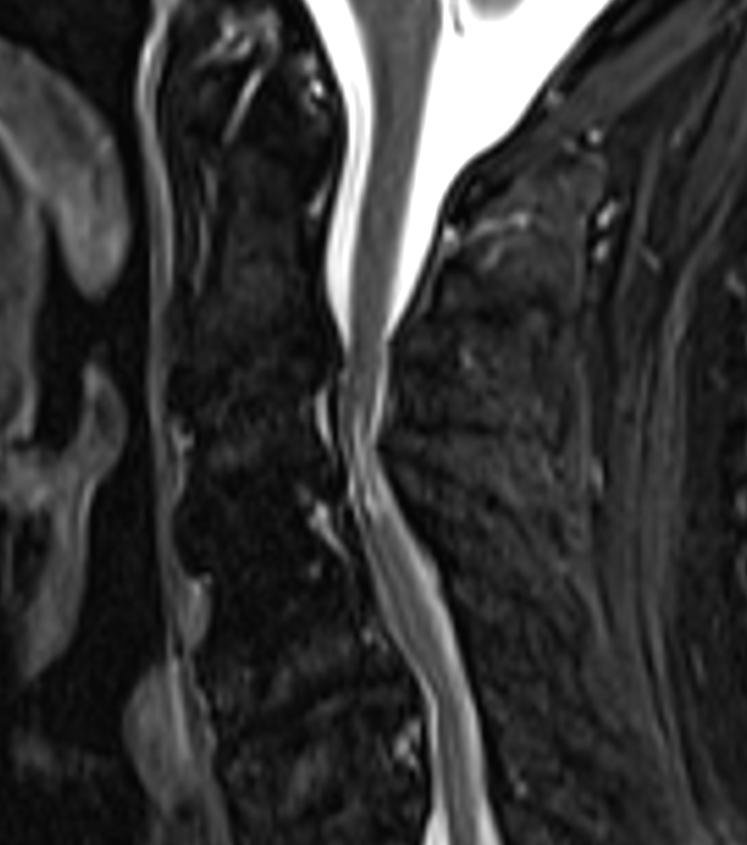
- Patient with prior compression of the cord due to spondylosis.
- The myelopathic segment is T2-hyperintense (particularly the grey matter) and small volume.
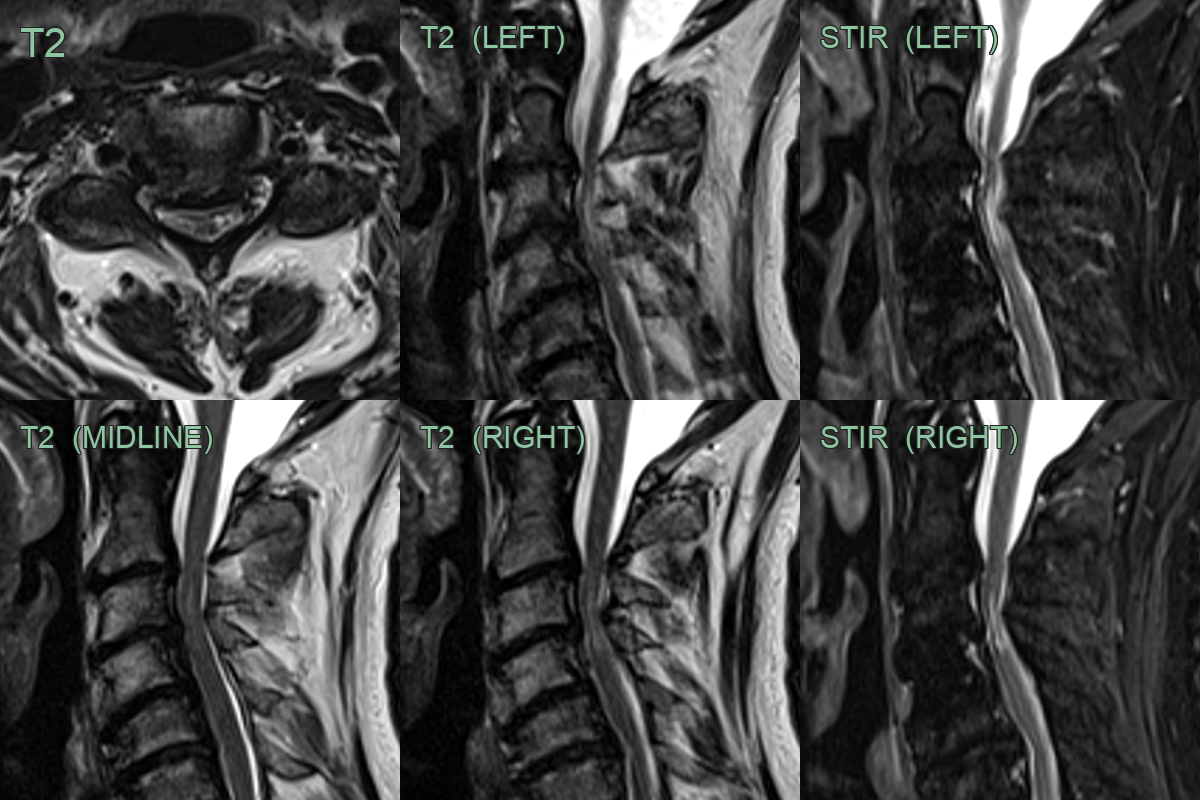
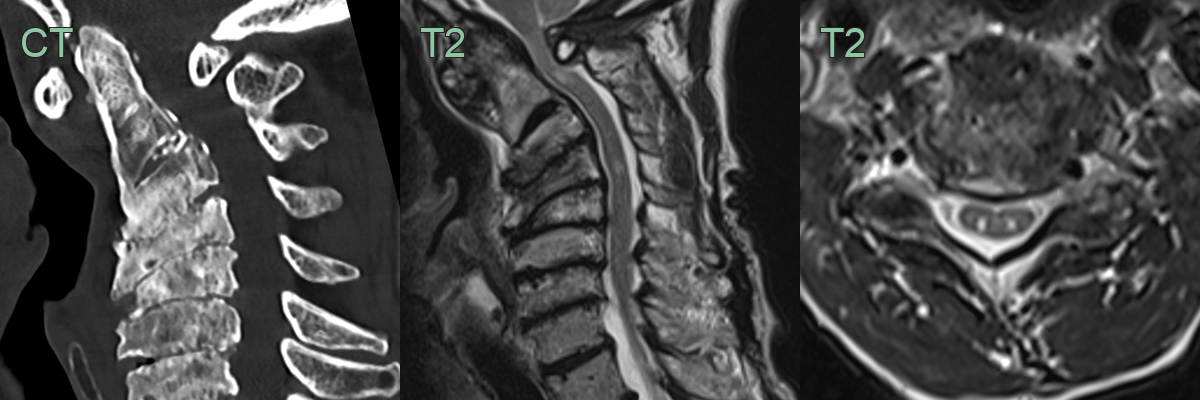
- 60-year-old patient with chronic myelopathic symptoms and severe bilateral upper limb radiculopathies.
- MRI showed posterior-osteophyte disc complexes causing moderately severe vertebral canal narrowing.
- The cord was atrophic and there was myelopathic signal change in the central and lateral cord.
Treatment¶
- Conservative management:
- Physical therapy
- Pain management
- Cervical collar or bracing
- Surgical interventions:
- Anterior cervical discectomy and fusion (ACDF)
- Laminectomy with or without fusion
- Corpectomy
- Tumour resection
- Emerging therapies:
- Stem cell transplantation
- Neuroprotective agents
- Neurotrophic factors
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Multiple sclerosis | Short (<3 vertebral segments) eccentric cord lesion on MRI; periventricular ovoid brain lesions; no structural compression |
| Transverse myelitis | Intramedullary T2 signal without structural compressive cause; cord expansion; no disc or bony pathology |
| Spinal cord infarction | Restricted diffusion on DWI; pencil-like anterior cord T2 signal; no compressive mass |
| Vitamin B12 deficiency | Posterior column T2 hyperintensity ("inverted V" sign); no structural compression; symmetric dorsal involvement |
| Syringomyelia | Central fluid-filled cavity on T2; follows CSF signal; may be associated with compressive cause |
| Spinal cord tumour | Intramedullary enhancing mass with cord expansion; no disc or bony compressive pathology |
| Radiation myelopathy | Located within prior radiation field; cord atrophy and T2 signal without compressive cause |
| Neuromyelitis optica spectrum disorder | Often associated with optic neuritis; NMO-IgG antibody positive |