Cortical Laminar Necrosis
Summary
- Cortical laminar necrosis (CLN) is a pattern of cerebral cortical injury characterised by selective necrosis of specific cortical layers
- Typically occurs due to severe hypoxia or ischaemia, often in the context of global hypoperfusion
- Imaging findings evolve over time, with characteristic gyriform T1 hyperintensity on MRI in subacute to chronic stages
Pathophysiology
- Results from energy failure and subsequent neuronal death in metabolically active cortical layers
- Most commonly affects layers 3 and 5, which have high metabolic demands
- Proposed mechanisms:
- Excitotoxicity from glutamate release
- Free radical formation
- Apoptosis
- Common causes:
- Hypoxic-ischaemic encephalopathy
- Status epilepticus
- Hypoglycaemia
- Carbon monoxide poisoning
Demographics
- Can occur at any age
- More commonly reported in:
- Neonates with hypoxic-ischaemic encephalopathy
- Adults with cardiac arrest or severe hypotension
- No clear gender predilection
Diagnosis
- Clinical presentation varies based on underlying cause and extent of injury
- Common symptoms:
- Altered mental status
- Focal neurological deficits
- Seizures
- Diagnosis often made on imaging, supported by clinical history
Imaging
- CT:
- Acute: Normal or subtle cortical hypodensity
- Subacute to chronic: Gyriform hyperdensity of affected cortex
- MRI:
- Acute (< 24 hours): Cortical diffusion restriction
- Subacute (> 2 weeks): Gyriform T1 hyperintensity
- T2/FLAIR: Variable signal, often hyperintense
- Contrast enhancement may occur
- Chronic: Cortical atrophy and gliosis
- Evolution of imaging findings:
- Diffusion restriction (acute)
- T1 hyperintensity (subacute to chronic)
- Atrophy and gliosis (chronic)
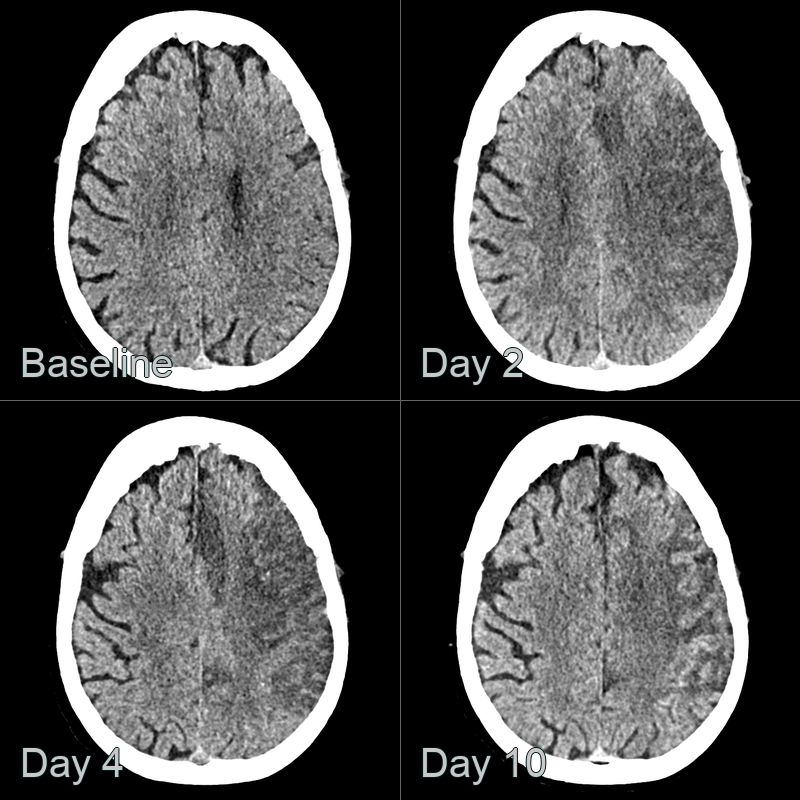
- A 50-year-old patient presented with right sided weakness.
- CT showed progressive hypoattenuation in the left MCA and ACA territory up to day 4.
- At day 10 post-admission, cortical hyperdensity (obsuring the ACA infarct) was consistent with cortical laminar necrosis.
Treatment
- No specific treatment for CLN itself
- Management focuses on:
- Treating underlying cause
- Supportive care and prevention of secondary injury
- Rehabilitation for neurological deficits
- Potential interventions:
- Neuroprotective strategies in acute phase (e.g., therapeutic hypothermia in neonatal hypoxic-ischaemic encephalopathy)
- Anticonvulsants for seizure control
- Physical, occupational, and speech therapy for functional recovery
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cerebral infarction | Follows vascular territory; CLN respects cortical layers |
| Encephalitis | Diffuse involvement; CLN is more localised to cortex |
| Hypoxic-ischaemic injury | More diffuse white matter involvement; CLN primarily affects cortex |
| Posterior reversible encephalopathy syndrome (PRES) | Predominantly affects posterior regions; CLN can occur anywhere |
| Status epilepticus | May show diffusion restriction; CLN shows T1 hyperintensity |
| Creutzfeldt-Jakob disease | Diffusion restriction in cortex and basal ganglia; CLN spares basal ganglia |
| Metastases | Nodular enhancement; CLN shows gyriform enhancement |
| Moyamoya disease | Involves deep white matter and basal ganglia; CLN is cortical |
| Cerebral venous thrombosis | Involves both gray and white matter; CLN is cortical |
| Mitochondrial encephalopathy | Involves basal ganglia; CLN spares deep gray matter |