Cortical Vein Thrombosis¶
Summary
- Rare form of cerebral venous thrombosis affecting superficial cortical veins
- Presents with focal neurological deficits, seizures, and headache
- Diagnosis confirmed by neuroimaging, with MRI and MRV being gold standard
Pathophysiology¶
- Thrombosis of cortical veins leads to:
- Localised venous congestion and oedema
- Potential haemorrhagic infarction
- Disruption of blood-brain barrier
- Underlying mechanisms:
- Hypercoagulable states
- Endothelial injury
- Venous stasis
Demographics¶
- Incidence: 1.32 per 100,000 person-years
- More common in:
- Women (3:1 female to male ratio)
- Young adults (median age 37 years)
- Risk factors:
- Pregnancy and puerperium
- Oral contraceptive use
- Thrombophilia
- Malignancy
- Dehydration
Diagnosis¶
- Clinical presentation:
- Focal neurological deficits (40-60%)
- Seizures (30-40%)
- Headache (70-90%)
- Laboratory tests:
- D-dimer (elevated in 94% of cases)
- Thrombophilia screening
- Neuroimaging:
- CT/CTA: may show hyperdense cortical veins, 'cord sign'
- MRI/MRV: gold standard for diagnosis
Imaging¶
- Non-contrast CT:
- Hyperdense cortical veins ('cord sign')
- Parenchymal oedema or haemorrhage
- CT venography:
- Filling defects in cortical veins
- MRI:
- T1: hyperintense thrombus in cortical veins
- T2*/SWI: 'blooming' artefact in thrombosed veins
- DWI: may show restricted diffusion in affected parenchyma
- MR venography:
- Absence of flow in affected cortical veins
- 'Tram-track' sign on contrast-enhanced images
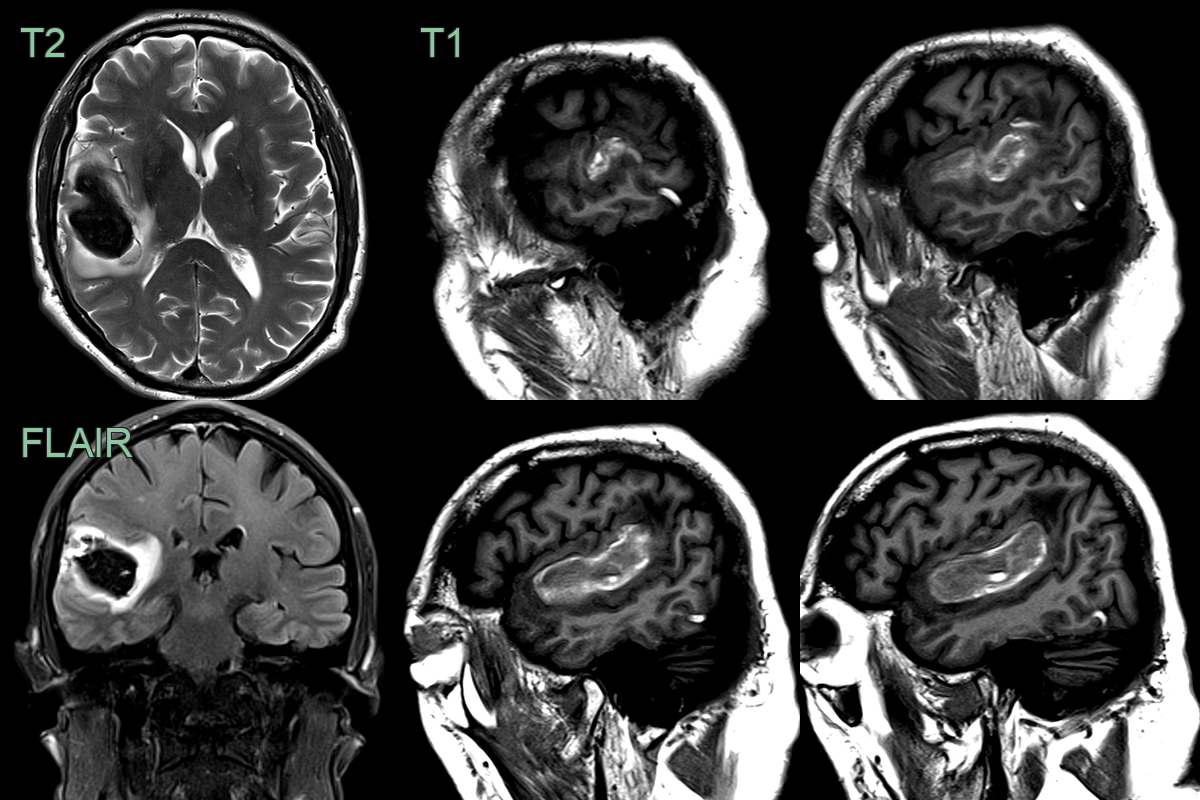
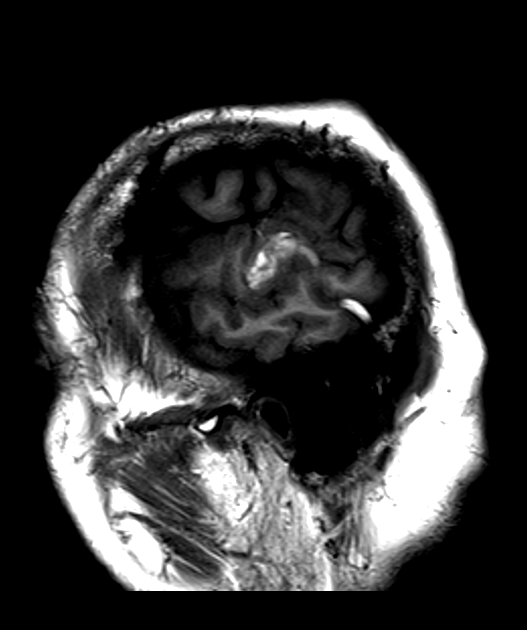
- A 60-year-old patient presented with a headache following a gastrointestinal illness.
- MRI showed a large haematoma centred on Heschl's gyrus.
- Serpigionous T1-hyperintensity over the temporal lobe represented acute thrombus in the vein of Labbe.
Treatment¶
- Anticoagulation:
- Low molecular weight heparin or unfractionated heparin
- Transition to oral anticoagulants (warfarin or direct oral anticoagulants)
- Duration: typically 3-12 months
- Supportive care:
- Seizure prophylaxis
- Management of intracranial pressure
- Endovascular intervention:
- Consider in severe cases refractory to medical management
- Mechanical thrombectomy or local thrombolysis
- Long-term follow-up:
- Monitor for recurrence and complications
- Address underlying risk factors
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Subarachnoid haemorrhage | Absence of "empty delta" sign on CT; different distribution of blood on imaging |
| Cerebral abscess | Ring-enhancing lesion with restricted central DWI; smooth thin capsule; no venous occlusion |
| Arterial ischaemic stroke | Arterial territory distribution; absence of haemorrhagic components in early stages |
| Tumour (e.g., glioma) | Mass effect; irregular enhancement pattern; absence of venous thrombosis on imaging |
| Reversible cerebral vasoconstriction syndrome | Thunderclap headache; "string of beads" appearance on angiography |
| Cerebral vasculitis | Multifocal infarcts; vessel wall enhancement on high-resolution MRI |
| Posterior reversible encephalopathy syndrome | Predominant posterior circulation involvement; reversible oedema |
| Encephalitis | Diffuse brain involvement outside of venous territory |