Craniopharyngioma¶
Summary
- Benign epithelial tumour arising from remnants of Rathke's pouch
- Typically presents with visual disturbances, endocrine dysfunction, and increased intracranial pressure
- Characteristic imaging findings include calcifications and cystic components in the sellar/suprasellar region
Pathophysiology¶
- Derived from embryonic remnants of Rathke's pouch
- Two histological subtypes:
- Adamantinomatous: More common in children, contains calcifications and cysts
- Papillary: More common in adults, typically solid
- Growth pattern:
- Slow-growing, but can cause significant local mass effect
- May invade adjacent structures, including hypothalamus and optic chiasm
Demographics¶
- Bimodal age distribution:
- Peak in children aged 5-14 years
- Second peak in adults aged 50-74 years
- Accounts for 2-5% of all primary intracranial tumours
- No significant gender predilection
Diagnosis¶
- Clinical presentation:
- Visual disturbances (e.g., bitemporal hemianopsia)
- Endocrine dysfunction (e.g., growth hormone deficiency, diabetes insipidus)
- Increased intracranial pressure (e.g., headaches, nausea, vomiting)
- Hormonal evaluation:
- Assessment of pituitary function (anterior and posterior)
- Ophthalmological examination:
- Visual field testing
- Visual acuity assessment
Imaging¶
- CT:
- Calcifications in 90% of adamantinomatous type
- Mixed solid and cystic components
- Hyperdense solid portions
- MRI:
- T1-weighted:
- Solid components: isointense to grey matter
- Cystic components: variable signal intensity
- T2-weighted:
- Solid components: isointense to hypointense
- Cystic components: hyperintense
- Post-contrast:
- Heterogeneous enhancement of solid portions
- Rim enhancement of cystic components
- Key imaging features:
- "Lobulated" appearance
- Calcifications (best seen on CT)
- Suprasellar extension with displacement of optic chiasm
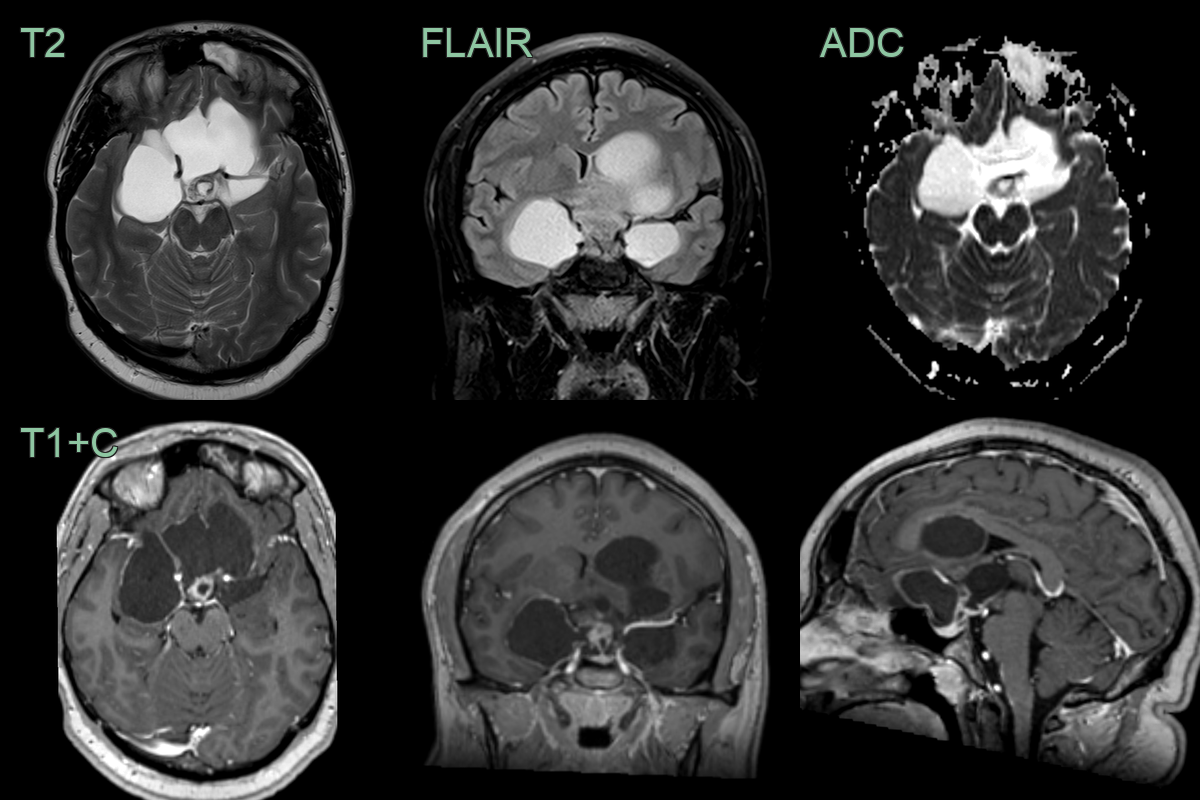
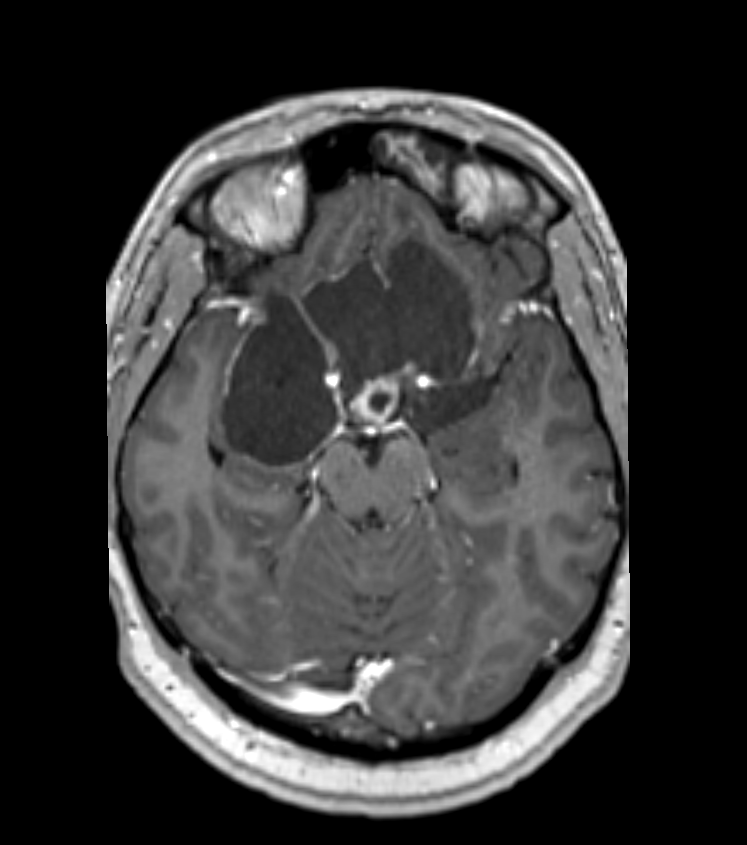
- A 20-year-old patient presented with a headache.
- MRI showed a partially enhancing suprasellar mass lesion with large cystic components.
Treatment¶
- Surgical resection:
- Primary treatment modality
- Gross total resection when feasible
- Challenges include proximity to critical structures
- Radiation therapy:
- Adjuvant treatment for residual tumour
- Stereotactic radiosurgery for small residual tumours
- Intracystic therapies:
- Bleomycin or interferon-alpha for recurrent cystic components
- Hormone replacement therapy:
- Management of endocrine dysfunction
- Long-term follow-up:
- Regular imaging surveillance
- Endocrine and ophthalmological monitoring
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pituitary adenoma | Typically homogeneous on MRI; rarely calcified |
| Rathke's cleft cyst | Unilocular cyst without solid component |
| Arachnoid cyst | No calcification; follows CSF signal on all sequences |
| Germ cell tumour | Typically midline; may have elevated tumour markers |
| Meningioma | Dural tail sign; homogeneous enhancement |
| Optic pathway glioma | Typically in children; involves optic chiasm/nerves |
| Hypothalamic glioma | Infiltrative appearance; rare calcification |
| Langerhans cell histiocytosis | Thickened pituitary stalk; diabetes insipidus common |
| Metastasis | Multiple lesions; known primary malignancy |
| Aneurysm | Flow voids on MRI; enhancement on angiography |