Cross Cerebellar Diaschisis¶
Summary

- Functional depression of the contralateral cerebellar hemisphere following a supratentorial lesion
- Characterised by reduced blood flow and metabolism in the cerebellar hemisphere opposite to a focal supratentorial lesion
- Typically associated with stroke but can occur in other conditions affecting cerebral cortex or subcortical structures
Pathophysiology¶
- Disruption of corticopontocerebellar pathway leads to deafferentation of the contralateral cerebellar hemisphere
- Reduced excitatory input from the cerebral cortex to the contralateral cerebellar hemisphere
- Results in decreased neuronal activity, blood flow, and metabolism in the affected cerebellar hemisphere
- Thought to be mediated by transneuronal metabolic depression rather than direct ischaemia
Demographics¶
- Most commonly observed in patients with acute ischaemic stroke
- Can occur in all age groups, but more frequent in older adults due to higher stroke incidence
- No significant gender predilection reported
- Also observed in traumatic brain injury, tumours, and epilepsy
Diagnosis¶
- Clinical diagnosis is challenging as symptoms may be masked by the primary supratentorial lesion
- Suspected in patients with:
- Acute stroke, especially in middle cerebral artery territory
- Large hemispheric lesions
- Subcortical white matter or basal ganglia involvement
- Definitive diagnosis relies on functional neuroimaging techniques
Imaging¶
- SPECT (Single Photon Emission Computed Tomography):
- Gold standard for diagnosis
- Shows decreased perfusion in the contralateral cerebellar hemisphere
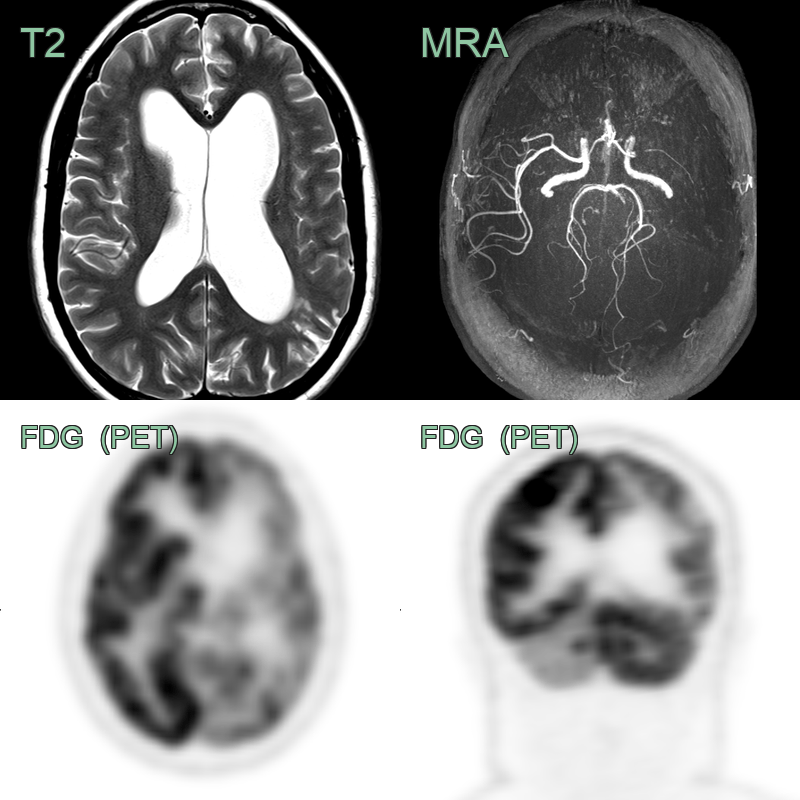
- PET (Positron Emission Tomography):
- Demonstrates reduced glucose metabolism in the affected cerebellar hemisphere
- CT perfusion:
- May show decreased blood flow in the contralateral cerebellar hemisphere
- MRI:
- Diffusion-weighted imaging (DWI) may show restricted diffusion in acute cases
- Arterial spin labeling (ASL) perfusion can demonstrate reduced cerebellar blood flow
- Conventional CT and MRI:
- Usually normal in the affected cerebellar hemisphere
- Useful for identifying the primary supratentorial lesion
Treatment¶
- No specific treatment for cross cerebellar diaschisis itself
- Management focuses on the underlying supratentorial lesion:
- Acute stroke treatment (thrombolysis, thrombectomy)
- Management of traumatic brain injury
- Treatment of tumours or epilepsy as appropriate
- Rehabilitation:
- Physical therapy and occupational therapy to address any cerebellar deficits
- Cognitive rehabilitation for associated cognitive impairments
- Prognosis:
- Often improves with resolution of the primary supratentorial lesion
- Persistent diaschisis may be associated with poorer functional outcomes
- Future directions:
- Research into potential neuroprotective strategies
- Investigation of targeted cerebellar stimulation techniques to improve outcomes
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cerebellar infarction | Restricted diffusion on DWI; does not cross midline |
| Posterior reversible encephalopathy syndrome (PRES) | Bilateral involvement, often in parieto-occipital regions |
| Cerebellar tumour | Mass effect, enhancement on contrast-enhanced MRI |
| Cerebellar abscess | Ring-enhancing lesion with restricted diffusion |
| Wernicke encephalopathy | Bilateral symmetrical involvement of mammillary bodies, thalami, and periaqueductal gray matter |
| Cerebellar atrophy | Generalized volume loss, not unilateral |
| Multiple sclerosis | Multiple white matter lesions, often ovoid and periventricular |
| Cerebellar contusion | Associated haemorrhagic foci on GRE/SWI; overlying skull fracture or extracranial soft tissue swelling on CT |
| Metastatic disease | Multiple lesions with surrounding oedema; ring or nodular enhancement; no ipsilateral supratentorial lesion |
| Spinocerebellar ataxia | Bilateral symmetric cerebellar and brainstem atrophy; no corresponding supratentorial lesion |