CSF1R-Related Leukoencephalopathy¶
Summary
- Rare genetic disorder affecting white matter of the brain
- Caused by mutations in the CSF1R gene
- Characterised by progressive cognitive decline, motor dysfunction, and psychiatric symptoms
Pathophysiology¶
- CSF1R gene mutations lead to dysfunction of microglia, the brain's primary immune cells
- Impaired microglial function results in:
- Reduced myelin maintenance and repair
- Accumulation of axonal spheroids
- Neuroinflammation and neurodegeneration
- Autosomal dominant inheritance pattern
Demographics¶
- Typically presents in adulthood (30-60 years)
- No significant gender predilection
- Rare disorder, exact prevalence unknown
- Reported cases predominantly in Caucasian populations, but may affect all ethnicities
Diagnosis¶
- Clinical presentation:
- Progressive cognitive decline
- Personality changes and psychiatric symptoms
- Motor dysfunction (e.g., gait disturbances, parkinsonism)
- Seizures (in some cases)
- Genetic testing:
- Identification of pathogenic variants in CSF1R gene
- Family history assessment
- Exclusion of other leukoencephalopathies
Imaging¶
- MRI findings:
- Bilateral, symmetrical white matter hyperintensities on T2-weighted and FLAIR sequences
- Predominant involvement of frontal and parietal lobes
- Corpus callosum atrophy
- Diffusion restriction in active lesions
- Calcifications in basal ganglia (in some cases)
- CT scan:
- May show hypodensities in affected white matter regions
- Calcifications in basal ganglia (if present)
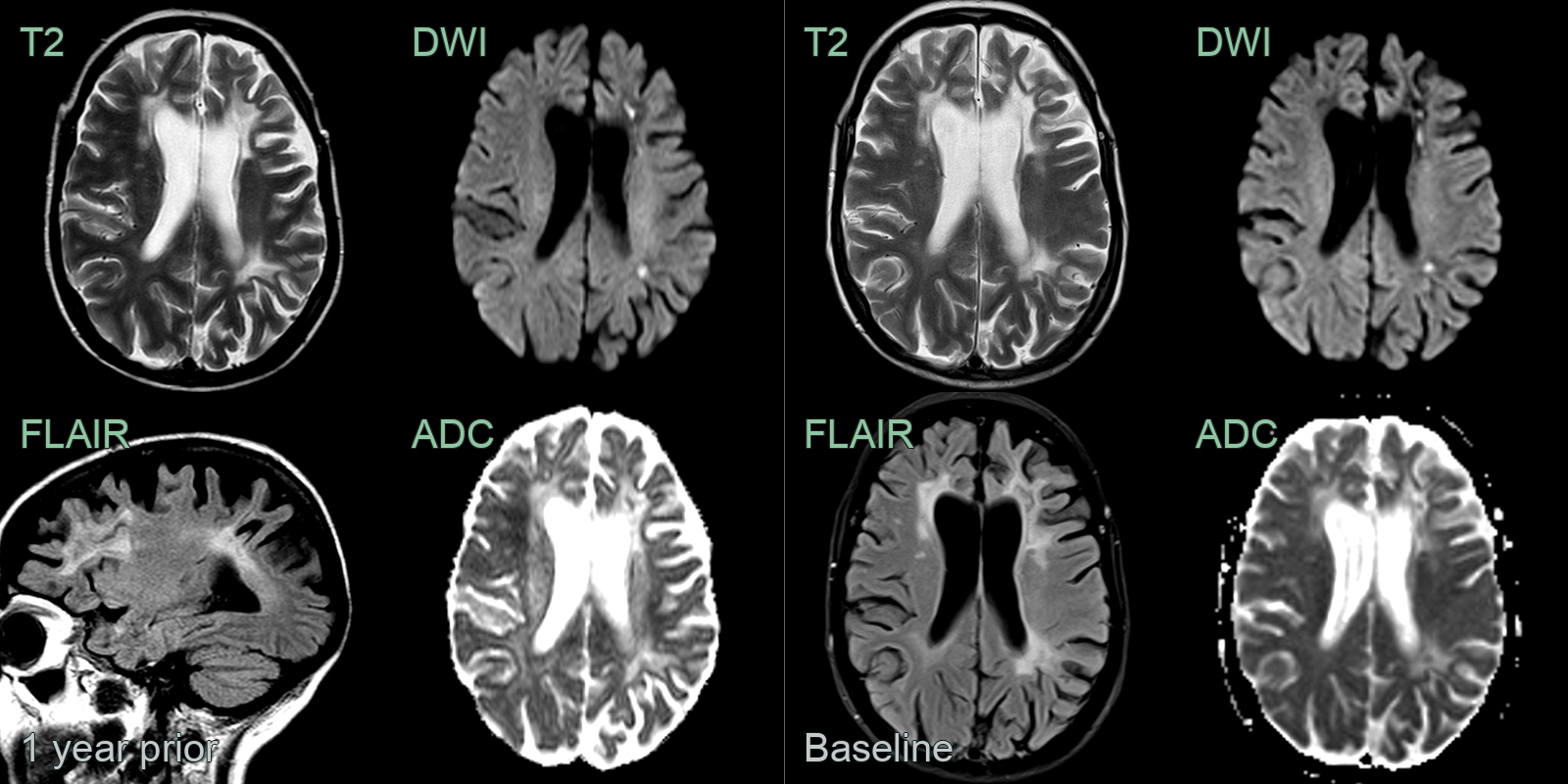
- A 50-year-old patient presented with behavioural change and low mood.
- MRI showed diffuse white matter hyperintensity, mainly in the frontal lobes, loss of white matter volume.
- Most characteristically, focal diffusion restriction persisted between the two scans that were 1 year apart.
Treatment¶
- No curative treatment available
- Management focuses on symptomatic relief and supportive care:
- Cognitive rehabilitation
- Physical therapy for motor symptoms
- Psychiatric medications for behavioural issues
- Anticonvulsants for seizure control (if present)
- Genetic counselling for affected individuals and family members
- Ongoing research into potential therapies:
- Haeatopoietic stem cell transplantation (experimental)
- CSF1R-targeted therapies (under investigation)
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Periventricular and juxtacortical lesions with Dawson fingers; ovoid morphology; lacks corpus callosum thinning |
| CADASIL | Temporal pole and external capsule involvement; subcortical lacunar infarcts |
| Cerebral vasculitis | Multifocal infarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI |