Dermoid Cyst¶
Summary
- Benign congenital lesion containing mature tissue derived from ectoderm, mesoderm, and endoderm
- Most commonly found in ovaries, but can occur anywhere along the midline of the body
- Imaging typically shows a cystic mass with fat-fluid levels and calcification
Pathophysiology¶
- Arise from trapped embryonic germ cells during fetal development
- Contain mature tissues such as:
- Hair follicles
- Sebaceous glands
- Sweat glands
- Teeth
- Bone
- Thyroid tissue
- Lined by keratinized squamous epithelium
- Slow-growing, but can rupture causing inflammation or malignant transformation (rare)
Demographics¶
- Most common in women of reproductive age (20-40 years)
- Ovarian dermoids account for 10-20% of all ovarian neoplasms
- Intracranial dermoids represent 0.5-1% of all intracranial tumours
- Can occur in both sexes and all age groups, but less common in men and children
Diagnosis¶
- Often asymptomatic and discovered incidentally
- Symptoms depend on location and size:
- Abdominal pain or pelvic pressure (ovarian dermoids)
- Headache, seizures, or focal neurological deficits (intracranial dermoids)
- Visible or palpable mass (cutaneous dermoids)
- Laboratory tests:
- Elevated CA-125 in some cases of ovarian dermoids
- Alpha-fetoprotein and beta-hCG to rule out germ cell tumours
Imaging¶
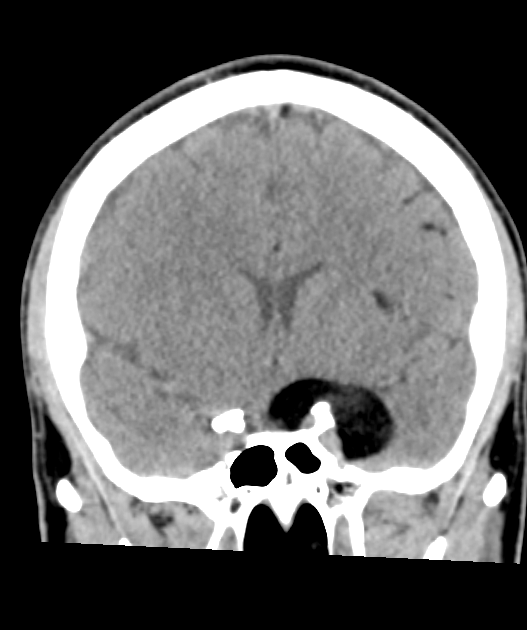
- CT:
- Fat-fluid levels
- Calcification
- Fat attenuation within lesion (-20 to -120 HU)
- MRI:
- T1-weighted: hyperintense fat components
- T2-weighted: variable signal intensity
- Fat suppressed sequences: useful for confirming fat content
- Chemical shift artefact at fat-fluid interface
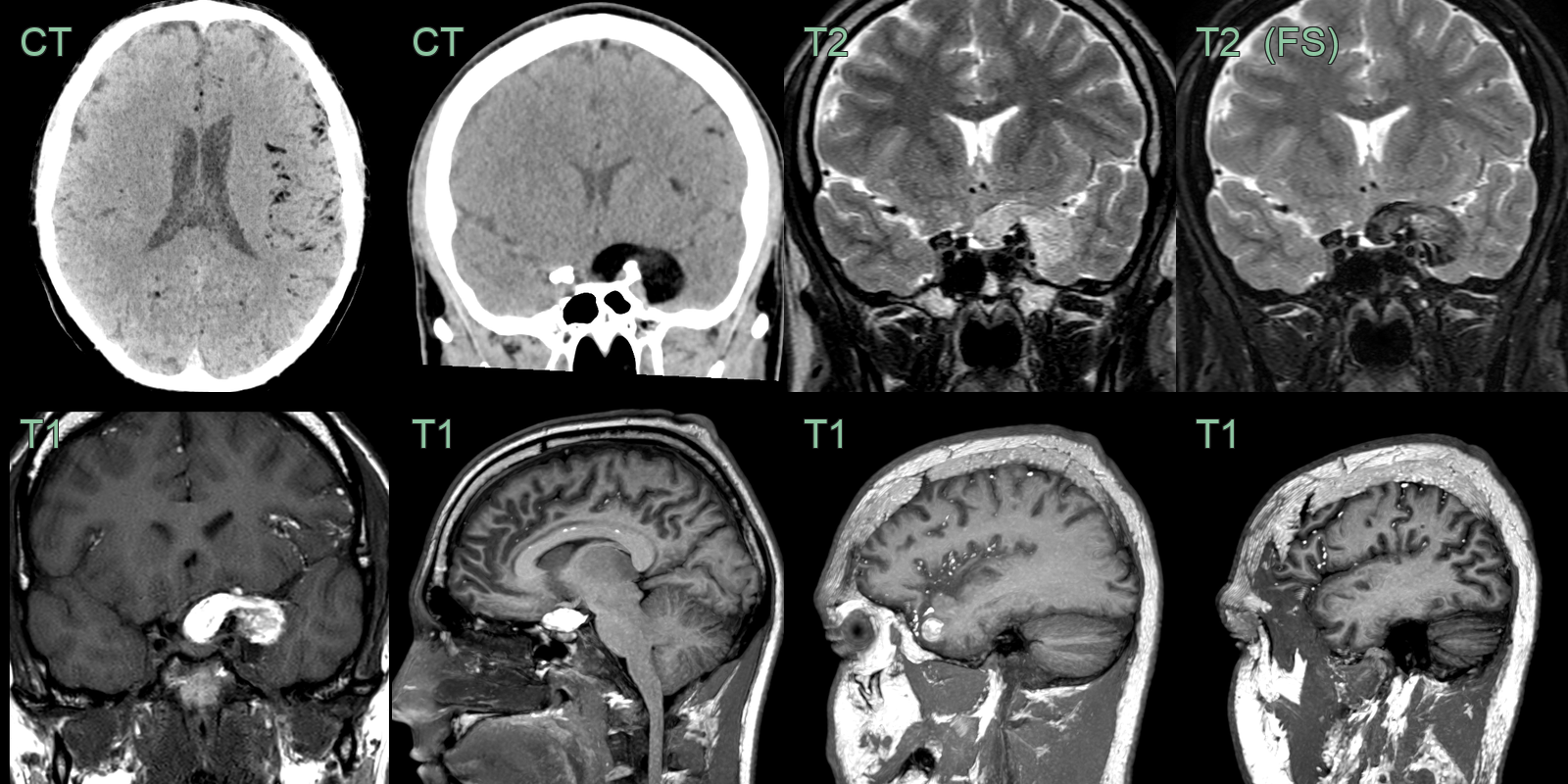

- A 30-year-old patient presented with an acute onset headache.
- MRI showed a lesion in the right cavernous sinus that was T1-hyperintense that suppressed on the fat-suppressed FLAIR imaging, consistent with fat content.
- There were further locules of fat signal over the cerebral hemispheres consistent with dermoid cyst rupture.
Treatment¶
- Surgical excision is the primary treatment
- Laparoscopic or open approach for ovarian dermoids
- Craniotomy for intracranial dermoids
- Simple excision for cutaneous dermoids
- Careful handling during surgery to prevent spillage and chemical peritonitis
- Fertility-sparing surgery for ovarian dermoids in young women
- Regular follow-up imaging for incompletely resected intracranial dermoids
- Malignant transformation is rare (<2%) but requires aggressive treatment if occurs
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Epidermoid cyst | Lacks dermal appendages on histology |
| Teratoma | Contains tissue from all three germ layers |
| Pilonidal cyst | Typically occurs in sacrococcygeal region |
| Lipoma | Homogeneous fat density on CT/MRI |
| Sebaceous cyst | Typically smaller and more superficial |
| Ganglion cyst | Lacks fat content, associated with joint or tendon sheath |
| Branchial cleft cyst | Located along anterior border of sternocleidomastoid muscle |
| Thyroglossal duct cyst | Moves with swallowing, midline neck location |
| Abscess | Surrounding inflammatory changes, no fat content |
| Lymphangioma | Fluid-filled spaces without fat content |