Developmental Venous Anomaly (DVA)¶
Summary
- DVAs are congenital vascular malformations characterised by a radial arrangement of dilated medullary veins converging on a large collecting vein
- Most common cerebral vascular malformation, typically asymptomatic and incidentally discovered on neuroimaging
- Generally considered benign and do not require treatment, but may rarely be associated with other vascular malformations or haemorrhage
Pathophysiology¶
- Result from arrested development of venous system during embryogenesis
- Represent persistent embryonic medullary veins that failed to regress
- Function as normal drainage pathways for brain parenchyma
- Typically drain into deep or superficial venous systems
Demographics¶
- Prevalence: 2.6% in autopsy series, up to 6.4% in MRI studies
- No significant gender predilection
- Can occur at any age, but most commonly diagnosed in adults
Diagnosis¶
- Usually asymptomatic and discovered incidentally on imaging
- Rarely associated with:
- Headaches
- Seizures
- Focal neurological deficits
- May coexist with other vascular malformations (e.g., cavernous malformations)
Imaging¶
- CT:
- Contrast-enhanced: "caput medusae" appearance of converging veins
- Non-contrast: may show calcifications or associated cavernomas
- MRI:
- T1-weighted: flow void of draining vein
- T2-weighted: hypointense radial veins
- Susceptibility-weighted imaging (SWI): prominent veins
- Post-contrast T1: enhancement of radial veins and draining vein
- Angiography:
- "Caput medusae" appearance in venous phase
- Normal arterial phase
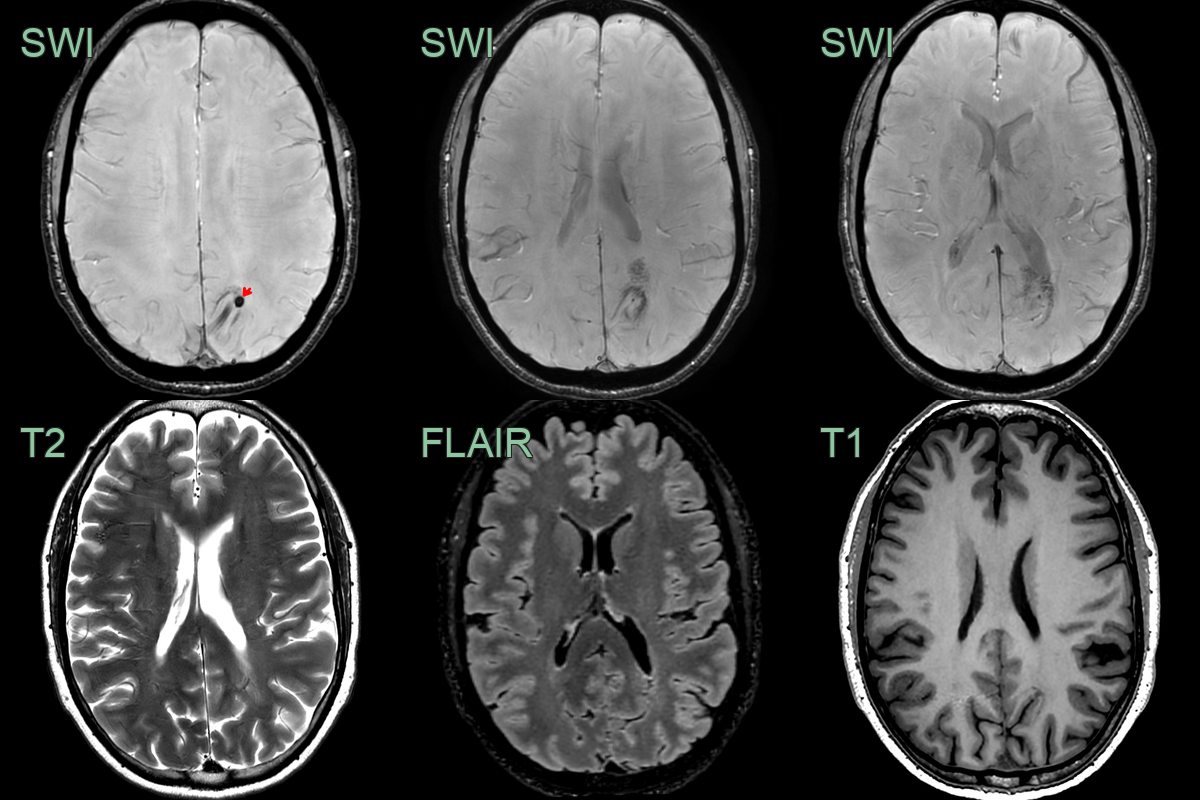
- Incidental findings of a dilated vein with the caput medusa sign.
- The DVA was associated with a small cavernoma (red arrow) .
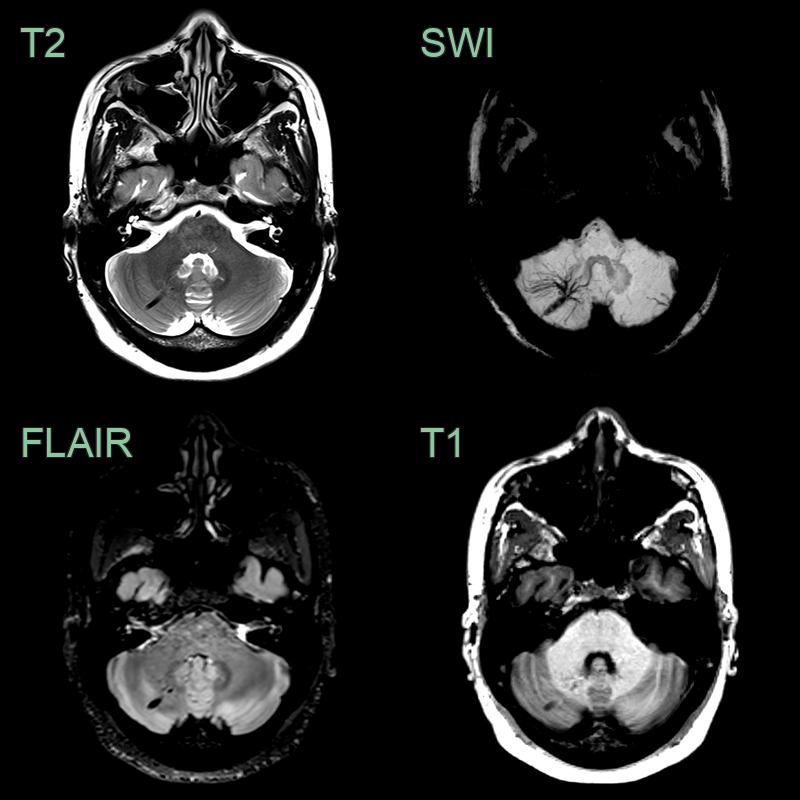
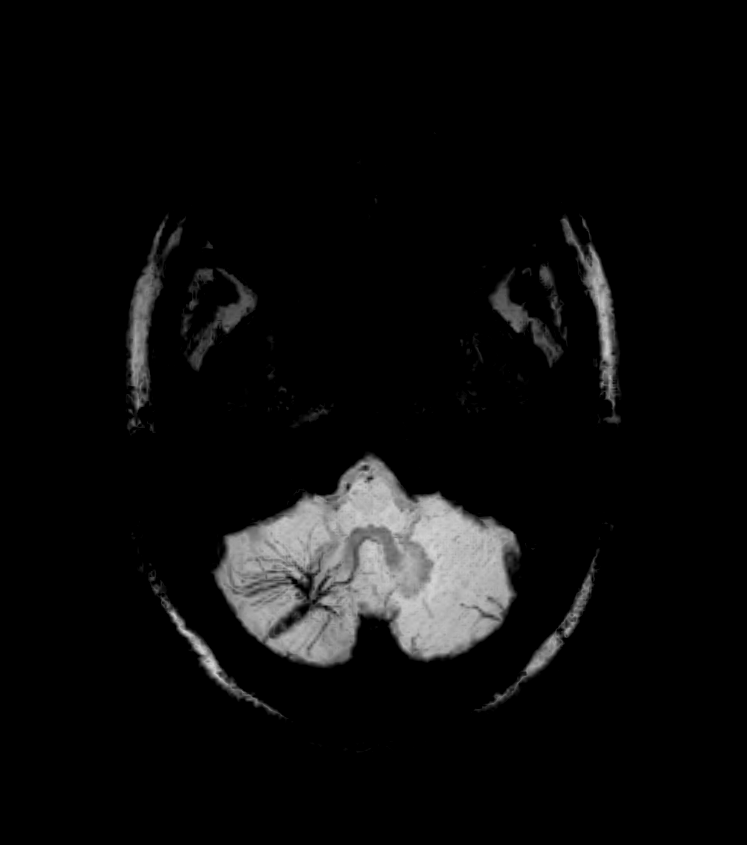
- Incidental finding of a flow void on all sequences with a wider caput medusae on the SWI minimum intensity projection.
Treatment¶
- Generally, no treatment required for asymptomatic DVAs
- Management focuses on associated conditions:
- Cavernous malformations: may require surgical resection
- Intracranial haemorrhage: conservative management or surgical intervention based on severity
- Anticoagulation should be used cautiously in patients with DVAs
- Surgical resection of DVAs is contraindicated due to risk of venous infarction
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cavernous Malformation | DVAs typically have a "caput medusae" appearance on contrast-enhanced imaging, while cavernous malformations have a popcorn-like appearance |
| Arteriovenous Malformation | DVAs do not show arterial feeders or early venous drainage on angiography, unlike AVMs |
| Capillary Telangiectasia | DVAs are larger and have a characteristic "umbrella" or "palm tree" appearance, while capillary telangiectasias are smaller and less organised |
| Dural Arteriovenous Fistula | DVAs do not demonstrate arterial-venous shunting or cortical venous reflux seen in dAVFs |
| Cerebral Aneurysm | DVAs do not show a saccular or fusiform dilatation of arteries, which is characteristic of aneurysms |
| Tumour (e.g., Glioma) | DVAs do not enhance or show mass effect like tumours, and they follow blood signal on all sequences |
| Cerebral Abscess | DVAs do not show restricted diffusion or ring enhancement typically seen in abscesses |
| Multiple Sclerosis Plaques | DVAs do not show the typical ovoid, periventricular white matter lesions seen in MS |
| Cerebral Infarction | DVAs do not show restricted diffusion or follow a vascular territory like acute infarcts |
| Cerebral Contusion | DVAs do not show blooming artefact on susceptibility-weighted imaging or evolve over time like contusions |