Diffuse Axonal Injury (DAI)¶
Summary
- Severe traumatic brain injury characterised by widespread damage to axons in white matter tracts
- Caused by rapid acceleration/deceleration or rotational forces to the head
- Imaging findings often subtle, with MRI being more sensitive than CT
Pathophysiology¶
- Primary injury:
- Shearing forces cause axonal stretching and disruption
- Cytoskeletal damage leads to impaired axonal transport
- Secondary injury:
- Delayed axotomy occurs hours to days after initial trauma
- Wallerian degeneration of affected axons
- Microglial activation and neuroinflammation
Demographics¶
- Most common in:
- Young adults (15-35 years)
- Males (3:1 male to female ratio)
- Main causes:
- Motor vehicle accidents
- Falls from height
- Assault
- Sports-related injuries (e.g., boxing, football)
Diagnosis¶
- Clinical presentation:
- Loss of consciousness at time of injury
- Prolonged coma or vegetative state
- Varying degrees of cognitive and motor impairment
- Glasgow Coma Scale (GCS) score:
- Often <8 (severe head injury)
- Biomarkers:
- Elevated serum levels of neuron-specific enolase (NSE) and S100B protein
Imaging¶
- Computed Tomography (CT):
- Limited sensitivity for DAI
- May show:
- Petechial haemorrhages in white matter
- Intraventricular or subarachnoid haemorrhage
- Associated contusions or mass effect
- Magnetic Resonance Imaging (MRI):
- Gold standard for DAI diagnosis
- Sequences:
- T2-weighted and FLAIR: hyperintense lesions in white matter
- Gradient Echo (GRE) or Susceptibility Weighted Imaging (SWI): haemorrhagic lesions
- Diffusion Weighted Imaging (DWI): acute axonal injury
- Adams grading system:
- Grade I: Corpus callosum involvement
- Grade II: Additional lesions in brainstem
- Grade III: Additional lesions in rostral brainstem
- Diffusion Tensor Imaging (DTI):
- Advanced technique for assessing white matter tract integrity
- Useful for prognostication and follow-up

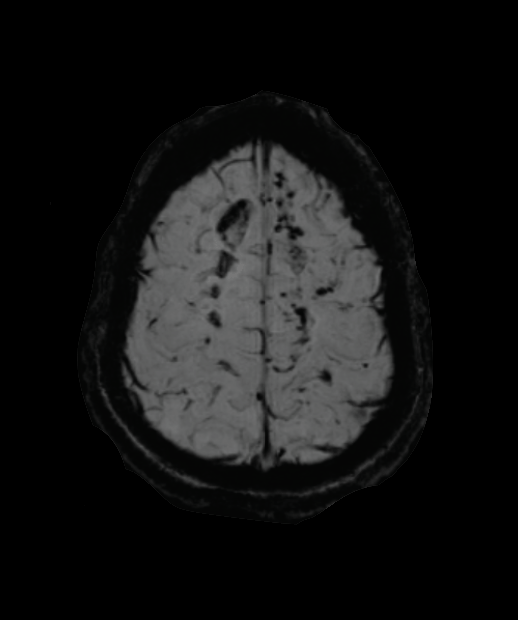
- 20-year-old male suffered a severe head injury following a skiing accident.
- T2-weighted imaging showed mature contusional damage at the vertex.
- SWI shows microhaemorrhages at the grey-white matter interface, corpus callosum and brainstem.
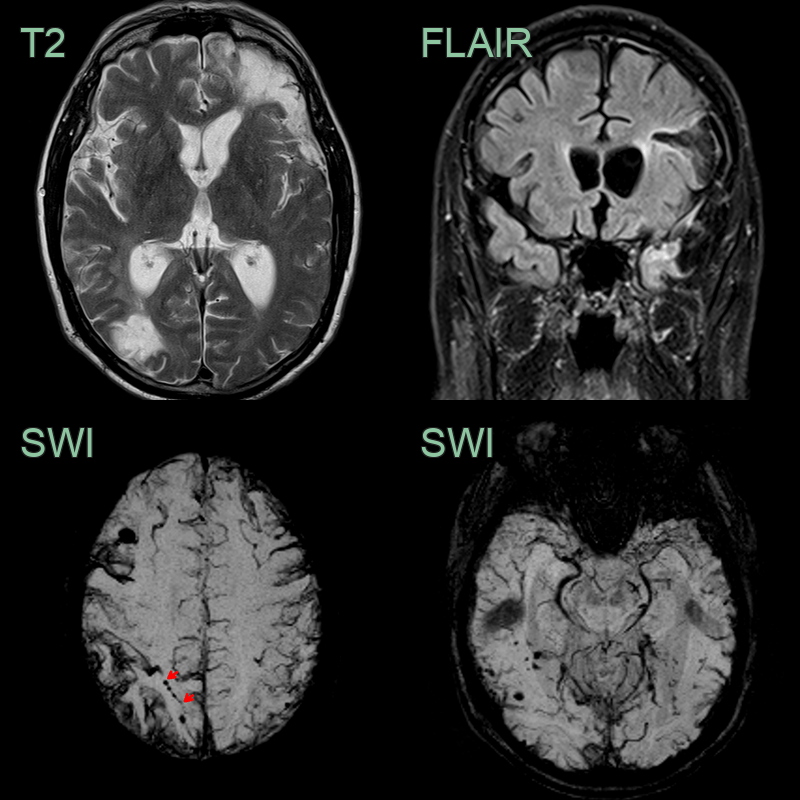
- A 50-year-old patient suffered a severe head injury following a road traffic accident 3 years prior to presentation within worsening cognition.
- MRI showed old parenchymal contusions in the left frontal and temporal lobes alongside an old contre-coup injury in the right occipital lobe.
- SWI showed extensive superficial cortical siderosis secondary to traumatic subarachnoid haemorrhage.
- There were many cortical or immediately subcortical microhaemorrhages. Some of the microhaemorrhages (e.g., in the right superior parietal lobe) were arranged linearly (red arrows).
Treatment¶
- Acute management:
- Intracranial pressure monitoring and management
- Maintenance of cerebral perfusion pressure
- Prevention of secondary injury (e.g., hypoxia, hypotension)
- Neuroprotective strategies:
- Hypothermia (controversial)
- Pharmacological interventions (e.g., progesterone, still under investigation)
- Rehabilitation:
- Multidisciplinary approach involving physiotherapy, occupational therapy, and speech therapy
- Cognitive rehabilitation
- Psychosocial support for patients and families
- Emerging therapies:
- Stem cell therapy (experimental)
- Neurotrophic factors to promote axonal regeneration
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Cerebral Contusion | Focal lesions on CT/MRI, typically in cortical areas |
| Subdural Haematoma | Crescent-shaped extra-axial collection on imaging |
| Hypoxic-Ischaemic Injury | More diffuse and symmetric brain involvement |
| Multiple Sclerosis | Periventricular white matter lesions, clinical history |
| Toxic Leukoencephalopathy | Exposure history, more symmetric white matter changes |
| Cerebral Oedema | Diffuse brain swelling without shear injury pattern |
| Traumatic Subarachnoid Haemorrhage | Blood in subarachnoid spaces on CT |
| Posterior Reversible Encephalopathy Syndrome (PRES) | Predominant posterior circulation involvement, reversible |
| Cerebral Fat Embolism | History of long bone fracture, starfield pattern on DWI |