Diffuse Hemispheric Glioma¶
Summary
- Rare, aggressive paediatric brain tumour characterised by diffuse infiltration of a cerebral hemisphere
- Typically presents with seizures, focal neurological deficits, and raised intracranial pressure
- MRI shows unilateral hemispheric involvement with T2/FLAIR hyperintensity and variable enhancement
Pathophysiology¶
- Classified as a WHO grade 4 glioma
- Often harbours H3 K27M mutations, similar to diffuse midline gliomas
- Characterised by rapid growth and infiltration of surrounding brain tissue
- Associated with poor prognosis due to its diffuse nature and resistance to treatment
Demographics¶
- Primarily affects children and young adults
- Peak incidence between 5-10 years of age
- Slight male predominance reported in some studies
- Rare, with exact incidence not well-established due to its recent recognition as a distinct entity
Diagnosis¶
- Clinical presentation:
- Seizures (focal or generalised)
- Progressive focal neurological deficits
- Signs of raised intracranial pressure (headache, vomiting, papilledema)
- Neuroimaging (MRI) is crucial for initial diagnosis
- Definitive diagnosis requires histopathological examination and molecular testing
Imaging¶
- MRI is the imaging modality of choice:
- T2/FLAIR: Diffuse hyperintensity involving a large portion of one cerebral hemisphere
- T1: Hypointense signal in the affected areas
- T1 post-contrast: Variable enhancement patterns, often minimal or absent
- DWI: May show areas of restricted diffusion
- MR spectroscopy: Elevated choline and reduced N-acetylaspartate peaks
- CT:
- May show subtle hypodensity and mass effect
- Calcifications are uncommon
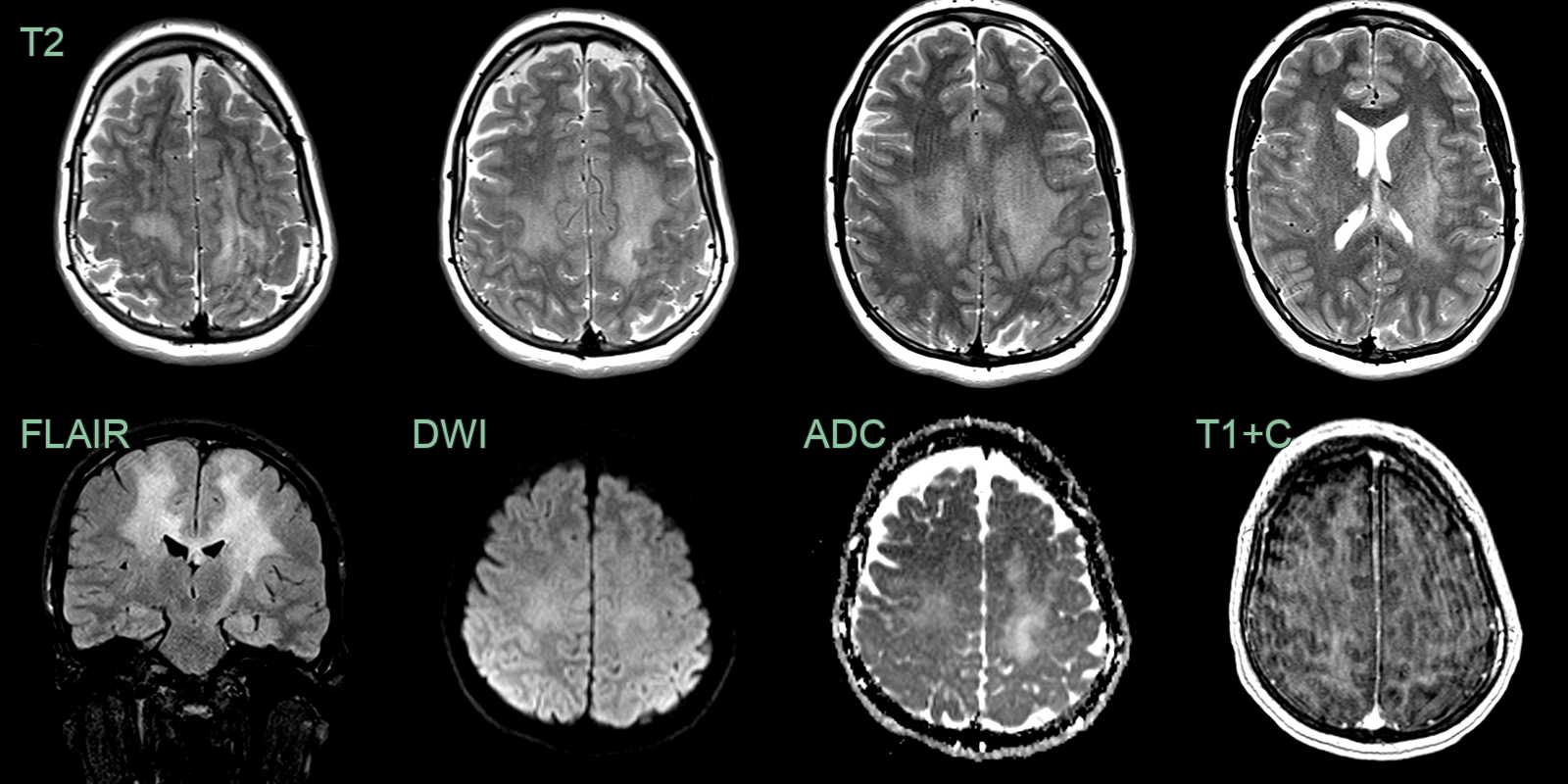
- A 20-year-old patient presented with rapidly progressive spasticity and ataxia.
- MRI showed diffuse bihemisheric ill-defined T2-weighted hyperintensity without diffusion restriction or enhancement.
- Biopsy revealed a H3 G34-mutant diffuse hemispheric glioma.
Treatment¶
- Multimodal approach, but prognosis remains poor
- Surgical resection:
- Often limited due to the diffuse nature of the tumour
- Aim to obtain tissue for diagnosis and reduce mass effect
- Radiotherapy:
- Focal or whole-brain radiation depending on extent of disease
- Dose-limiting in young children due to neurocognitive risks
- Chemotherapy:
- Various regimens used, including temozolomide and nitrosoureas
- Limited efficacy due to the blood-brain barrier and drug resistance
- Targeted therapies:
- Under investigation, including BRAF inhibitors for BRAF-mutated tumours
- Supportive care:
- Anti-epileptic drugs for seizure control
- Corticosteroids for managing oedema and raised intracranial pressure
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Acute disseminated encephalomyelitis (ADEM) | Diffuse bilateral white matter and basal ganglia involvement; no progressive mass effect; no H3K27M imaging correlate |
| Multiple sclerosis | Periventricular ovoid lesions; "Dawson's fingers" on sagittal FLAIR; no hemispheric mass effect |
| Lymphoma | Homogeneous enhancement; periventricular; restricted diffusion; hyperdense on non-contrast CT |
| Metastatic disease | Multiple lesions at grey-white junction; ring or nodular enhancement; surrounding vasogenic oedema |
| Vasculitis | Multifocal cortical and subcortical infarcts in multiple territories; vessel wall enhancement on high-resolution MRI |
| Progressive multifocal leukoencephalopathy (PML) | Subcortical U-fibre involvement; no enhancement; restricted diffusion at active edge; no mass effect |
| Leukodystrophy | Symmetric white matter involvement; specific patterns (anterior, posterior, or central) depending on type |
| Encephalitis | Cortical and limbic T2 signal; often bilateral temporal involvement; may show restricted DWI in active areas |
| Posterior reversible encephalopathy syndrome (PRES) | Posterior-predominant vasogenic oedema; elevated ADC; no hemispheric mass |
| Glioblastoma | Prominent central necrosis with irregular ring enhancement; more established mass effect |