Diffuse Midline Glioma¶
Summary

- Aggressive, infiltrative brain tumour typically affecting children and young adults
- Characterised by a specific histone H3 mutation (H3K27M)
- Poor prognosis with median survival of 9-12 months despite treatment
Pathophysiology¶
- Arises from glial cells in midline structures of the brain
- H3K27M mutation leads to epigenetic dysregulation and altered gene expression
- Infiltrative growth pattern with diffuse spread along white matter tracts
- Often associated with oedema and mass effect
Demographics¶
- Peak incidence in children and young adults (median age 5-11 years)
- Slight male predominance (male:female ratio 1.14:1)
- Accounts for 10-20% of all paediatric brain tumours
- Rare in adults, but can occur
Diagnosis¶
- Clinical presentation:
- Depends on tumour location (e.g., brainstem, thalamus, spinal cord)
- Common symptoms: cranial nerve palsies, ataxia, hemiparesis, headache
- Histopathology:
- WHO grade 4 glioma
- Immunohistochemistry positive for H3K27M mutation
- Molecular testing:
- Confirmation of H3K27M mutation in H3F3A or HIST1H3B/C genes
Imaging¶
- MRI is the imaging modality of choice
- T1-weighted imaging:
- Hypointense to isointense mass
- Variable enhancement pattern (often minimal or heterogeneous)
- T2-weighted and FLAIR imaging:
- Hyperintense mass with infiltrative appearance
- Surrounding oedema and mass effect
- Diffusion-weighted imaging:
- Variable restricted diffusion
- MR spectroscopy:
- Elevated choline, reduced N-acetylaspartate
- Presence of lactate and lipid peaks
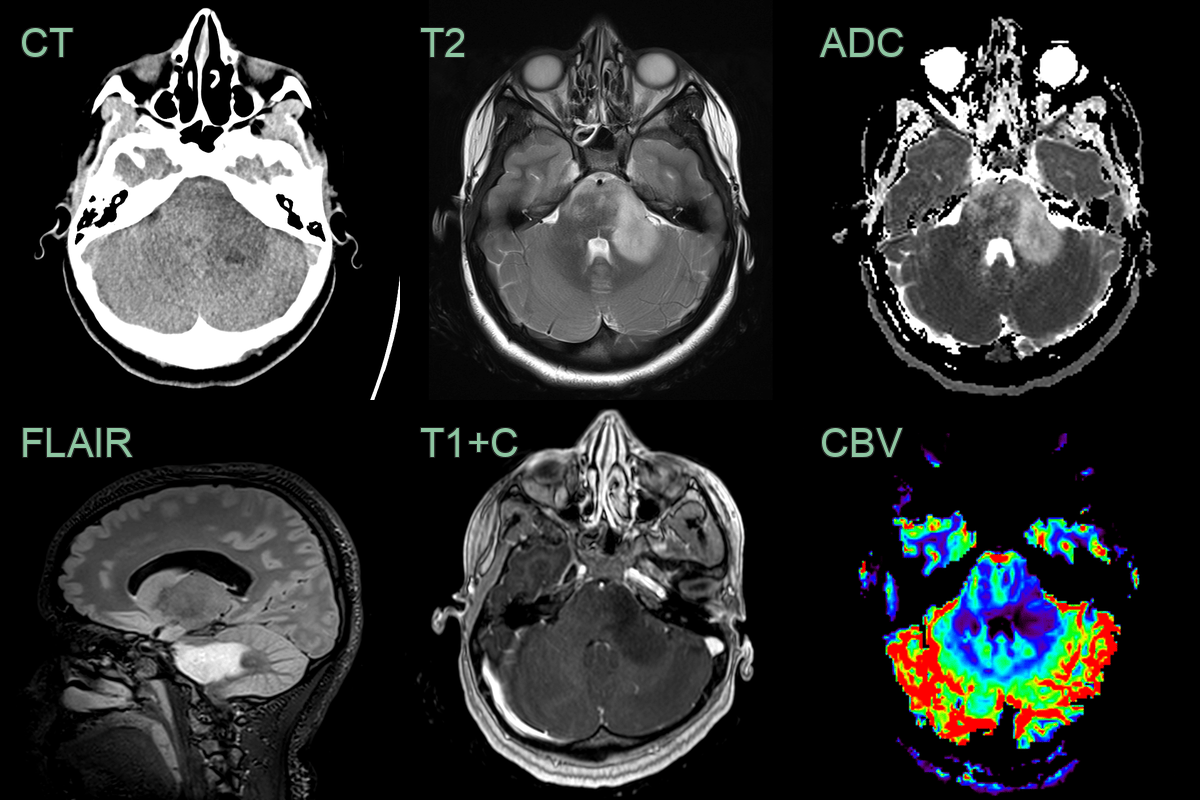
- 20-year-old patient presetned with headaches, blurred vision, nausea and vomitting.
- MRI showed a diffuse T2-hyperintense lesion centred in a mildly expanded cerebellar peduncle.
- Lower ADC values, potentially representing areas of higher celluarity, corresponded to a region of mildly increased rCBV (1.4 relative to the contralateral side).
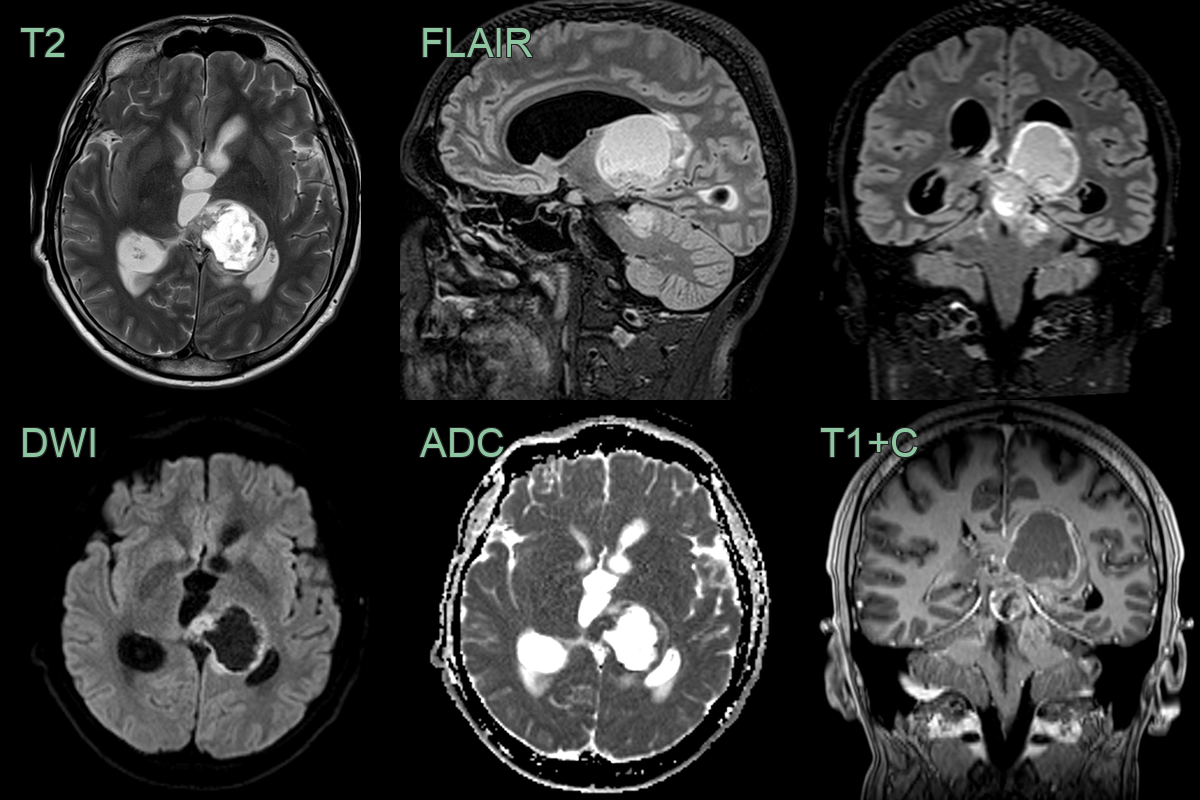
- 20-year-old patient presented with acute onset headache.
- MRI showed a acute obstructive hydrocephalus secondary to a solid-cystic lesion centred on the left thalamus.
- Low ADC values within the solid and enhancing component of the tumour indicated hyperceullarity.
- Biopsy revealed a H3 K27M-mutant diffuse midline glioma.
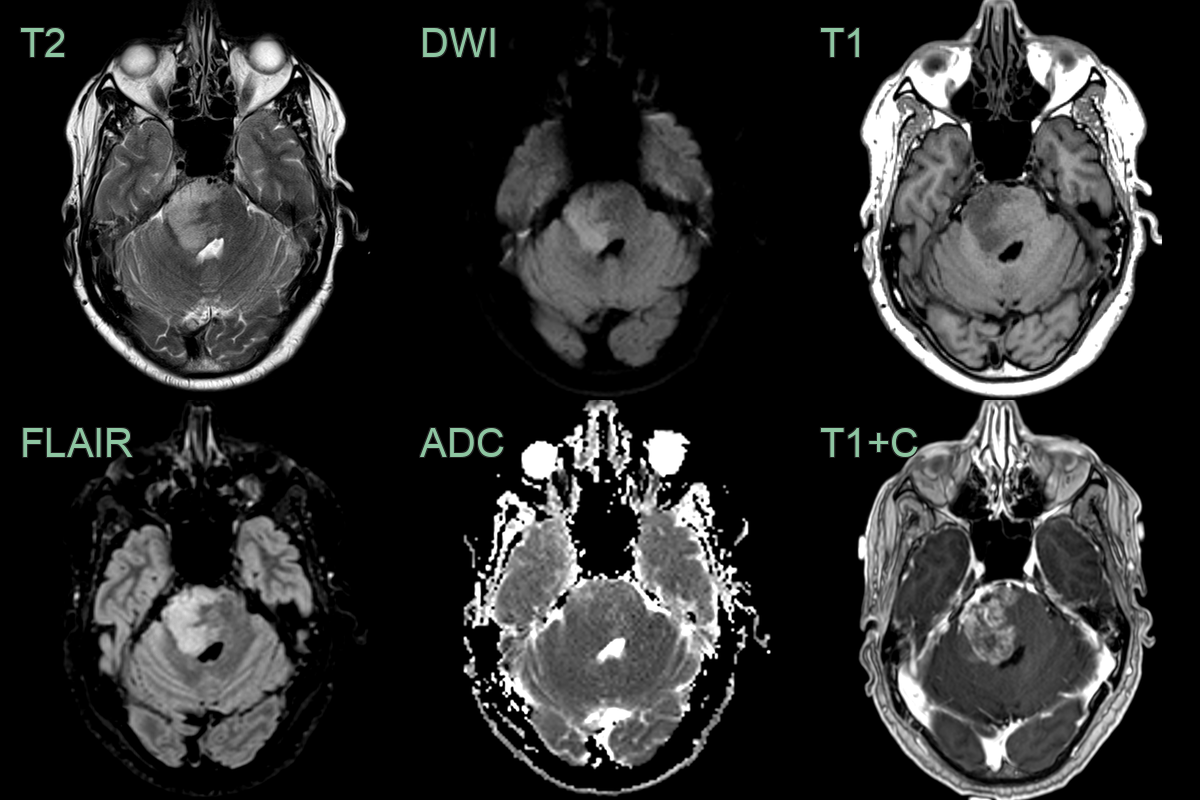
- A 55-year-old patient presented with headache, nausea and vomitting.
- MRI showed an enhancing lesion in the right side of the pons with slightly reduced ADC values.
- Given an extensive travel history the imaging differential included both neoplasta and infection/inflammation.
- Biopsy revealed an H3 K27M-mutant diffuse midline glioma.
Treatment¶
- Multimodal approach with limited efficacy
- Surgical options:
- Often limited due to eloquent location
- Biopsy for diagnosis and molecular testing
- Radiotherapy:
- Standard fractionated radiotherapy (54-60 Gy)
- Re-irradiation may be considered at recurrence
- Chemotherapy:
- Temozolomide (limited efficacy)
- Ongoing trials with targeted therapies (e.g., HDAC inhibitors, PARP inhibitors)
- Supportive care:
- Corticosteroids for oedema management
- Anticonvulsants for seizure control
- Novel approaches under investigation:
- Immunotherapy (e.g., checkpoint inhibitors)
- Convection-enhanced delivery of targeted agents
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pilocytic Astrocytoma | Typically well-circumscribed, cystic appearance on MRI |
| Medulloblastoma | Usually located in the cerebellum, enhances more homogeneously |
| Ependymoma | Often has calcifications, may have cystic components |
| Brainstem Encephalitis | Patchy T2 signal without diffuse expansion of the pons; may enhance; often involves multiple brainstem levels |
| Pontine Tegmental Cap Dysplasia | Characteristic "molar tooth" appearance on axial MRI; congenital; associated with curved superior cerebellar peduncles |
| Demyelinating Disease | Multiple lesions including supratentorial; ovoid periventricular plaques; no diffuse brainstem expansion |
| Metastatic Tumour | Ring or nodular enhancement; multiple lesions; no diffuse T2 brainstem expansion |
| Lymphoma | Typically enhances more homogeneously, often multiple lesions |
| Primitive Neuroectodermal Tumour (PNET) | Usually more heterogeneous, may have cystic/necrotic areas |
| Ganglioglioma | Often has calcifications, less invasive appearance |