Discitis¶
Summary

- Inflammatory condition affecting the intervertebral disc space and adjacent vertebral endplates
- Typically presents with severe back pain, fever, and neurological symptoms
- Diagnosis relies on clinical presentation, laboratory findings, and imaging studies, particularly MRI
Pathophysiology¶
- Usually results from hematogenous spread of infection to the avascular intervertebral disc
- Common causative organisms:
- Staphylococcus aureus (most frequent)
- Streptococcus species
- Escherichia coli
- Mycobacterium tuberculosis (in endemic areas)
- Infection leads to:
- Inflammation of the disc space
- Destruction of cartilaginous endplates
- Potential spread to adjacent vertebral bodies
Demographics¶
- Can affect all age groups, but bimodal distribution:
- Young children (< 5 years)
- Adults > 50 years
- Risk factors:
- Immunocompromised states
- Intravenous drug use
- Recent spinal surgery or invasive procedures
- Diabetes mellitus
- Chronic renal failure
Diagnosis¶
- Clinical presentation:
- Severe, localised back pain
- Fever (may be absent in chronic cases)
- Neurological deficits (in advanced cases)
- Laboratory findings:
- Elevated inflammatory markers (ESR, CRP)
- Leukocytosis
- Microbiological studies:
- Blood cultures (positive in 50-70% of cases)
- CT-guided biopsy for culture and sensitivity
Imaging¶
- Plain radiographs:
- Often normal in early stages
- Later findings: disc space narrowing, endplate erosions, vertebral body destruction
- Computed Tomography (CT):
- Better visualisation of bony changes
- Useful for guiding biopsy procedures
- Magnetic Resonance Imaging (MRI):
- Modality of choice for early diagnosis and follow-up
- Findings:
- T1-weighted: low signal intensity in disc space and adjacent vertebral bodies
- T2-weighted: high signal intensity in disc space and adjacent vertebral bodies
- Contrast enhancement of disc space and adjacent vertebral bodies
- Potential epidural or paraspinal abscesses
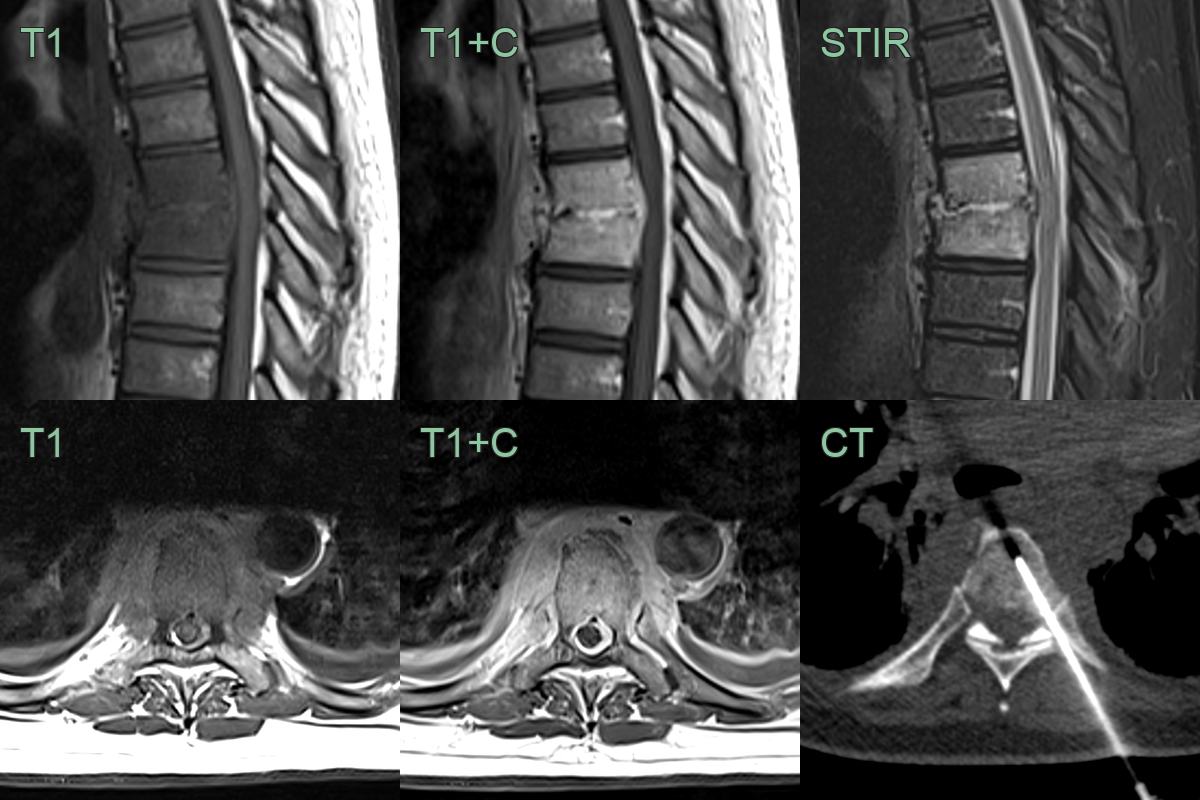
- A 60-year-old patient presented was midtoracic back pain with elevated inflammatory markers.
- MRI showed enplate erosion, vertebral body oedema and enhancing paraspinal soft tissue.
- Discitis secondary to Staphlococcus Aureus infection was diagnosed based on blood culture and CT-guided biopsy.
Treatment¶
- Antimicrobial therapy:
- Empiric broad-spectrum antibiotics initially
- Tailored based on culture and sensitivity results
- Prolonged course (6-12 weeks) typically required
- Conservative management:
- Bed rest and immobilisation in early stages
- Gradual mobilisation as symptoms improve
- Surgical intervention:
- Indicated for:
- Neurological deficits
- Spinal instability
- Failure of conservative treatment
- Procedures may include:
- Debridement and fusion
- Abscess drainage
- Pain management:
- Analgesics and anti-inflammatory medications
- Follow-up:
- Regular clinical and radiological assessment to monitor treatment response
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Degenerative disc disease | Disc space narrowing with osteophytes and vacuum disc phenomenon on CT; no T1 hypointensity or STIR hyperintensity crossing the disc space |
| Vertebral compression fracture | Vertebral body height loss without disc space involvement or end-plate erosion; preserved disc signal |
| Spinal metastasis | Focal vertebral body lesions without crossing the disc space; preserved disc height; T1 hypointense and STIR hyperintense |
| Epidural abscess | Rim-enhancing epidural collection separate from disc; posterior epidural location; may occur without disc involvement |
| Osteomyelitis without discitis | Vertebral body involvement without significant disc signal change or end-plate erosion |
| Ankylosing spondylitis | Shiny corners and syndesmophytes on CT; sacroiliac joint fusion; no fluid signal crossing disc space |
| Herniated disc | Disc protrusion with preserved end-plate signal; no T1 or STIR signal change in adjacent vertebral bodies |
| Spinal tuberculosis | Gibbus deformity; paraspinal and psoas abscess with rim enhancement; relative preservation of disc until late stage |