Drop Metastases¶
Summary
- Drop metastases are secondary tumour deposits that occur along the neuraxis due to seeding via cerebrospinal fluid (CSF)
- Most commonly associated with primary brain tumours, particularly medulloblastoma and ependymoma
- Imaging plays a crucial role in diagnosis and follow-up, with MRI being the modality of choice
Pathophysiology¶
- Occurs when tumour cells detach from a primary intracranial or intraspinal neoplasm and spread via CSF pathways
- Gravity-dependent distribution along the neuraxis, particularly in the lumbosacral region
- Tumour cells adhere to and infiltrate the leptomeninges, forming nodular or diffuse deposits
Demographics¶
- Most common in paediatric patients with primary brain tumours
- Medulloblastoma: 30-40% risk of drop metastases
- Ependymoma: 10-15% risk of drop metastases
- Less common in adults, but can occur with high-grade gliomas and other primary CNS tumours
Diagnosis¶
- Clinical presentation:
- Often asymptomatic in early stages
- May present with radiculopathy, myelopathy, or cauda equina syndrome
- CSF analysis:
- Cytology may reveal malignant cells
- Elevated protein levels
- Imaging is essential for definitive diagnosis
Imaging¶
- MRI is the gold standard for detection and characterisation:
- T1-weighted sequences with gadolinium enhancement
- T2-weighted and FLAIR sequences
- Key imaging findings:
- Nodular or linear enhancing lesions along the spinal cord or cauda equina
- Leptomeningeal enhancement
- Hydrocephalus may be present due to CSF obstruction
- Whole neuraxis imaging is crucial for comprehensive evaluation
- CT myelography may be used if MRI is contraindicated
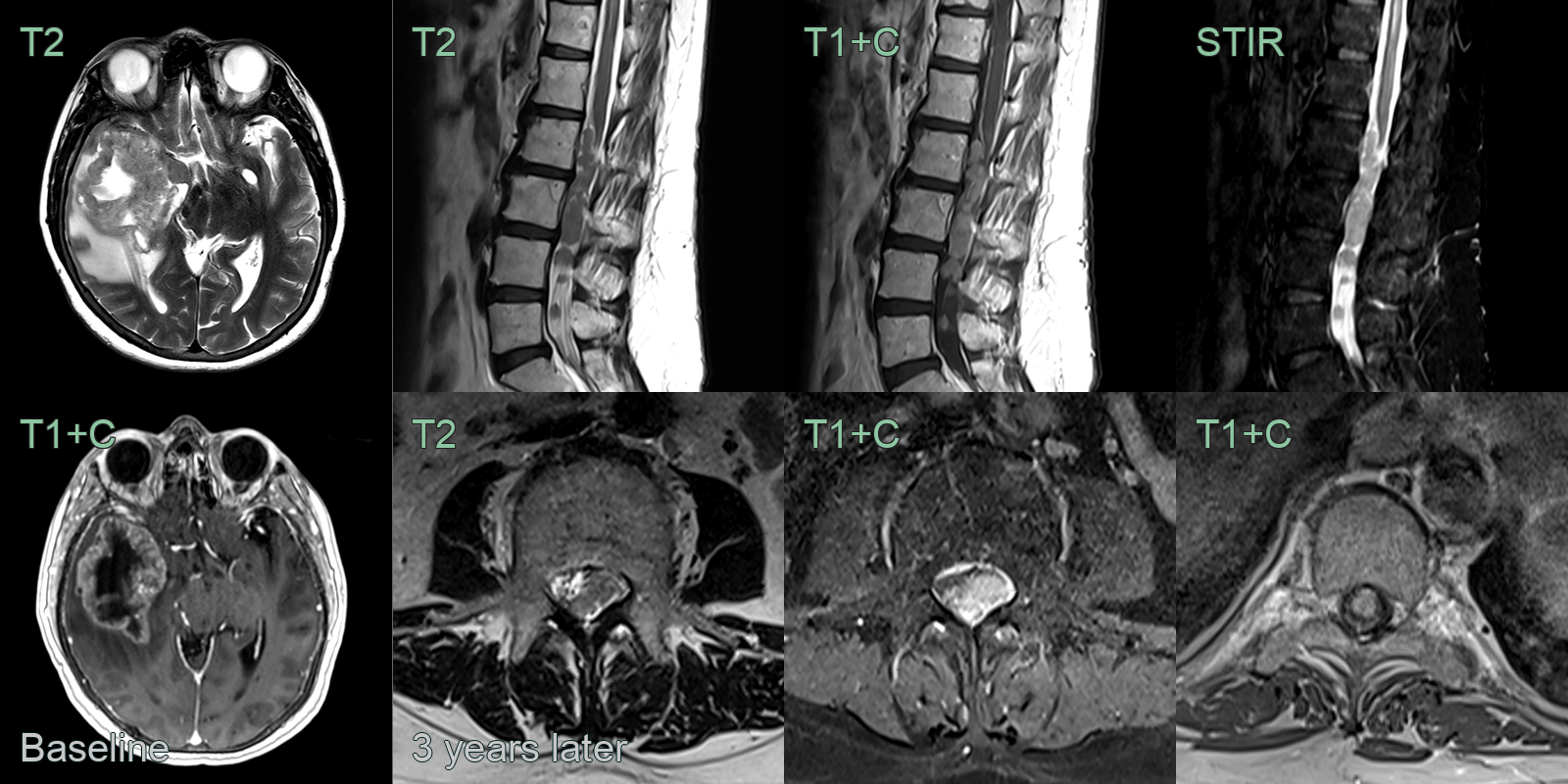
- A 60-year-old patient presented with headache and was diagnosed with solitary cerebral metastasis from a breast primary.
- The patient was stable for 3 years following resection and chemoradiotherapy.
- 3 years after the initial presentation, the patient re-presented with lower limb weakness. MRI showed a large volume of compressive drop metastases in the lumbar and thoracic region.
Treatment¶
- Multidisciplinary approach involving neurosurgery, oncology, and radiation therapy
- Treatment options:
- Surgical resection of accessible lesions
- Craniospinal irradiation
- Intrathecal chemotherapy
- Systemic chemotherapy
- Prognosis is generally poor, with median survival ranging from 2-6 months
- Regular follow-up imaging is essential to monitor treatment response and detect recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Leptomeningeal carcinomatosis | Diffuse smooth or nodular pial enhancement along cord surface and cranial nerves; no discrete nodular intradural masses |
| Spinal cord ependymoma | Intramedullary location; cap sign (haemosiderin) on T2; associated syrinx; expansile cord |
| Neurosarcoidosis | Leptomeningeal and root enhancement; dorsal subpial T2 signal; associated parenchymal lesions and cranial nerve involvement |
| Spinal meningioma | Single dural-based enhancing lesion with dural tail; broad base; no nodular root deposits |
| Spinal schwannoma | Enhancing intradural extramedullary mass at nerve root exit zone; may have dumbbell morphology through foramen |
| Arachnoiditis | Clumped and adherent nerve roots on MRI; peripheral tethering to dural sac; no discrete enhancing nodules |
| Primary CNS lymphoma | Intra-axial location; homogeneous enhancement; restricted diffusion; periventricular predilection |
| Tuberculosis (spinal) | Associated vertebral body involvement and end-plate erosion; rim-enhancing paraspinal or psoas abscess |