Dural Arteriovenous Fistula
Summary
- Abnormal connection between dural arteries and venous sinuses or cortical veins
- Presents with pulsatile tinnitus, headache, or intracranial haemorrhage
- Diagnosed by catheter angiography; treated with endovascular embolisation or surgery
Pathophysiology
- Acquired lesions resulting from:
- Venous sinus thrombosis
- Trauma
- Surgery
- Hypercoagulable states
- Classified by Cognard or Borden systems based on venous drainage pattern
- Increased risk of intracranial haemorrhage with cortical venous drainage
Demographics
- Incidence: 0.15-0.29 per 100,000 person-years
- Peak age: 50-60 years
- Slight female predominance
- Higher incidence in postmenopausal women and pregnancy
Diagnosis
- Clinical presentation:
- Pulsatile tinnitus
- Headache
- Intracranial haemorrhage
- Seizures
- Neurological deficits
- Bruit on auscultation over mastoid or orbit
- Catheter angiography: gold standard for diagnosis and classification
Imaging
- CT:
- Nonspecific findings
- May show dilated vessels, venous sinus thrombosis, or haemorrhage
- CT angiography:
- Demonstrates abnormal arterial feeders and early venous filling
- Limited in detecting small fistulas
- MRI:
- Flow voids representing enlarged vessels
- T2 hyperintensity in white matter (venous congestion)
- Susceptibility-weighted imaging: prominent cortical veins
- MR angiography:
- Time-of-flight and contrast-enhanced techniques
- Shows abnormal arterial feeders and early venous filling
- Catheter angiography:
- Definitive diagnosis and classification
- Identifies arterial feeders, fistula location, and venous drainage pattern
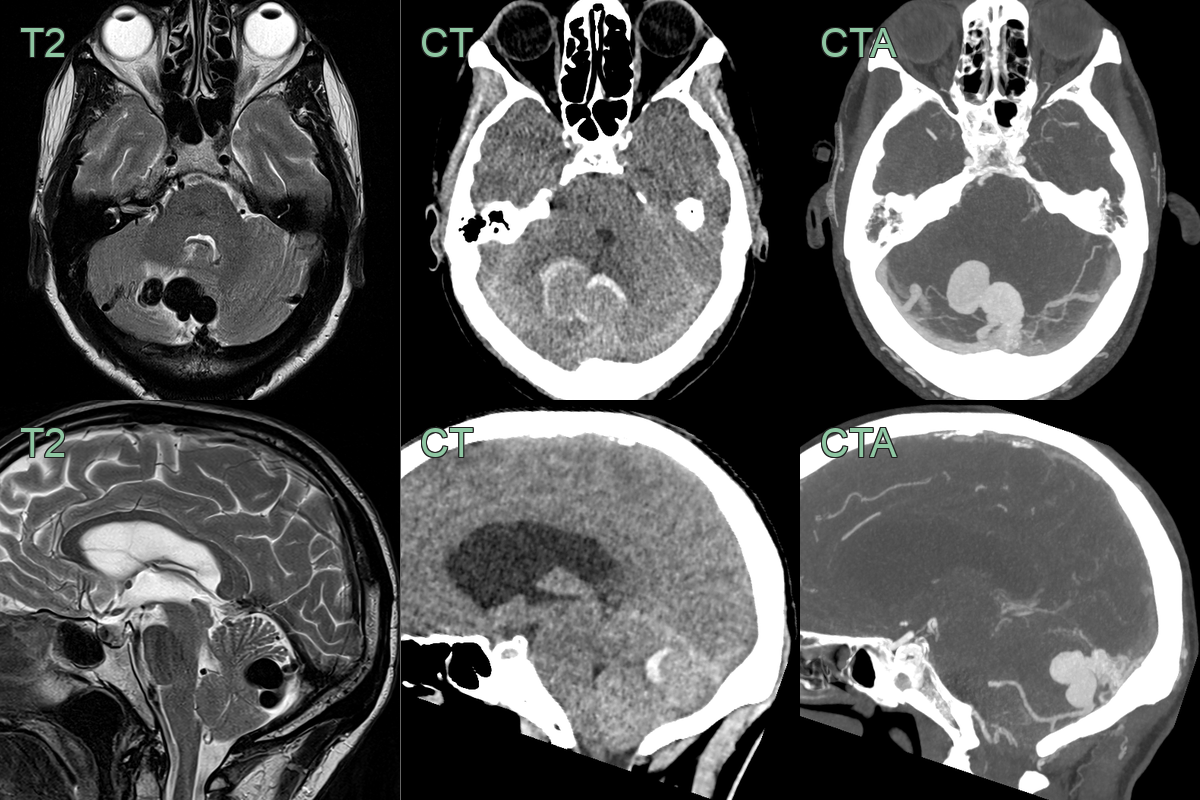
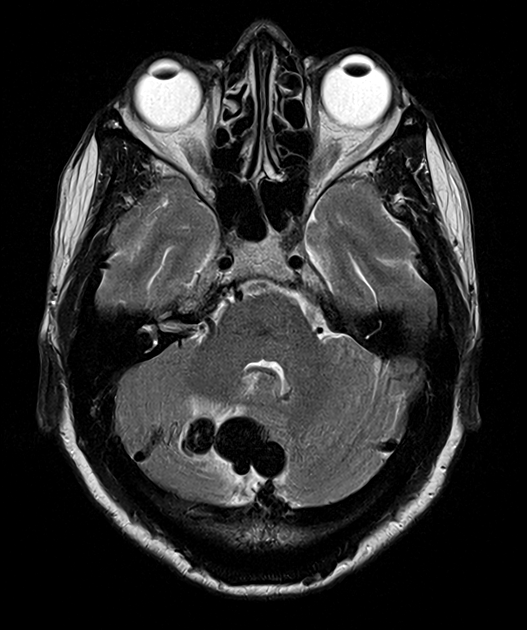
- A 60-year-old patient presented with headache.
- An MRI on admission showed a dilated vessel in the posterior fossa with a rim of oedema within the cerebellum.
- Immediately after the MRI, the patient's headache worsened and an CTA showed haemorrhage around the dural arteriovenous fistula that was supplied by the PICA.
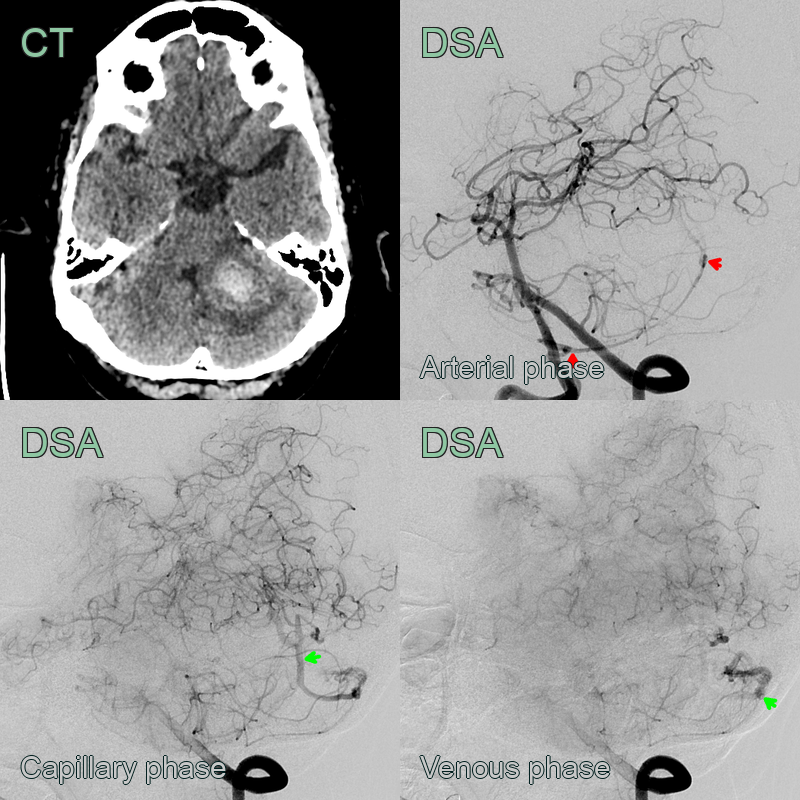
- A 60-year-old patient presented with headache and ataxia.
- The arterial phase of the DSA showed an abnormal vessel arising from the PICA draining into a dilated vein.
Treatment
- Conservative management for low-risk fistulas (Cognard type I, IIa)
- Endovascular embolisation:
- First-line treatment for most cases
- Transarterial or transvenous approach
- Materials: coils, liquid embolic agents (Onyx, n-BCA)
- Microsurgical resection:
- Reserved for complex cases or endovascular failures
- Direct exposure and disconnection of fistula
- Stereotactic radiosurgery:
- Adjunctive treatment or for small, surgically inaccessible fistulas
- Delayed occlusion (1-3 years)
- Follow-up imaging:
- MRI/MRA or catheter angiography to assess treatment response and recurrence
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Arteriovenous Malformation | Lacks direct arterial-venous shunting; has intervening nidus |
| Cavernous Malformation | Lacks arterial feeders; characteristic "popcorn" appearance on MRI |
| Venous Angioma | Single large draining vein; no arterial component |
| Capillary Telangiectasia | Enhances on MRI but no flow voids; no arterial feeders |
| Pial Arteriovenous Fistula | Located in brain parenchyma, not dural space |
| Tumour (e.g., meningioma) | Solid mass effect; different enhancement pattern |
| Cerebral Aneurysm | Focal dilatation of artery; lacks abnormal arteriovenous shunting |
| Moyamoya Disease | Bilateral steno-occlusive changes; characteristic "puff of smoke" appearance |
| Sinus Thrombosis | Filling defect in dural sinus; lacks arterial feeders |
| Sturge-Weber Syndrome | Leptomeningeal angiomatosis; calcifications; usually in children |