Dural Venous Sinus Thrombosis¶
Summary
- Dural venous sinus thrombosis (DVST) is a rare cerebrovascular disorder characterised by thrombosis of the dural sinuses and/or cerebral veins
- Clinical presentation varies widely, from isolated headache to severe neurological deficits
- Imaging plays a crucial role in diagnosis, with MRI and MR venography being the gold standard
Pathophysiology¶
- Thrombosis of dural sinuses and/or cerebral veins leads to:
- Increased venous pressure
- Decreased cerebrospinal fluid absorption
- Increased intracranial pressure
- Potential venous infarction and haemorrhage
- Common sites of thrombosis:
- Superior sagittal sinus
- Transverse sinus
- Sigmoid sinus
- Straight sinus
- Hypercoagulable states, infections, and mechanical factors contribute to DVST
Demographics¶
- Incidence: 1.32-1.57 per 100,000 person-years
- More common in women (3:1 ratio)
- Peak incidence in third decade of life
- Risk factors:
- Pregnancy and puerperium
- Oral contraceptives
- Thrombophilia
- Malignancy
- Infections (e.g., mastoiditis, sinusitis)
- Dehydration
Diagnosis¶
- Clinical presentation:
- Headache (most common symptom, present in >90% of cases)
- Focal neurological deficits
- Seizures
- Altered mental status
- Papilledema
- Laboratory tests:
- D-dimer (elevated in most cases, but normal levels do not exclude DVST)
- Thrombophilia workup
- Lumbar puncture:
- Increased opening pressure
- Normal or mildly abnormal CSF composition
Imaging¶
- CT:
- Non-contrast CT:
- Dense triangle sign (hyperdense thrombus in superior sagittal sinus)
- Empty delta sign (contrast-enhanced CT)
- CT venography:
- Filling defects in dural sinuses
- MRI and MR venography (gold standard):
- T1-weighted: Isointense to hyperintense thrombus
- T2-weighted: Variable signal intensity
- Susceptibility-weighted imaging (SWI): Hypointense thrombus
- Diffusion-weighted imaging (DWI): Restricted diffusion in venous infarcts
- MR venography:
- Flow voids in affected sinuses
- Collateral venous channels
- Digital subtraction angiography (DSA):
- Reserved for cases with equivocal MRI/MRV findings or when endovascular treatment is considered
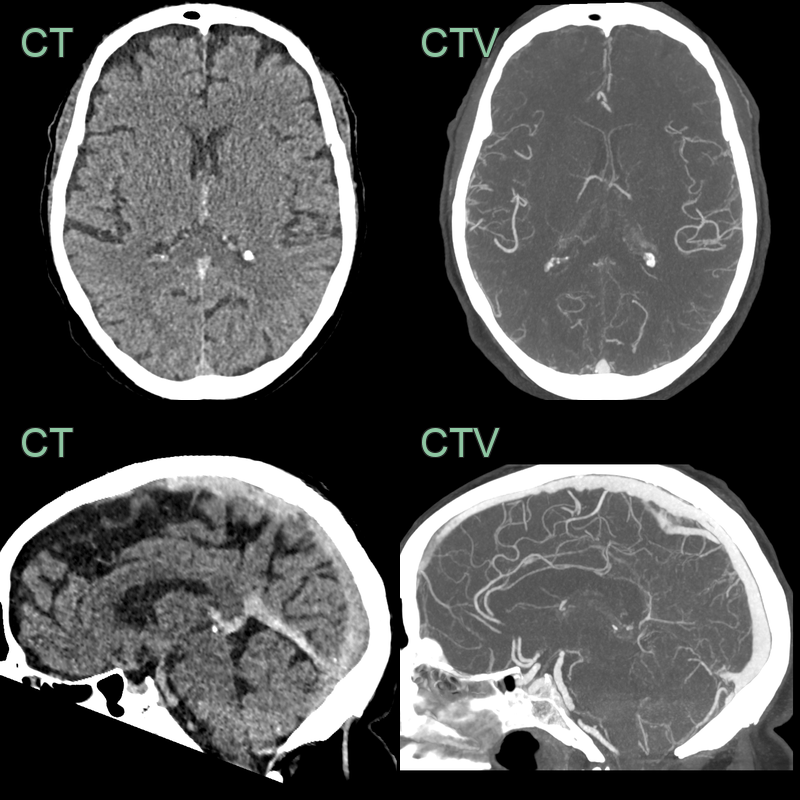
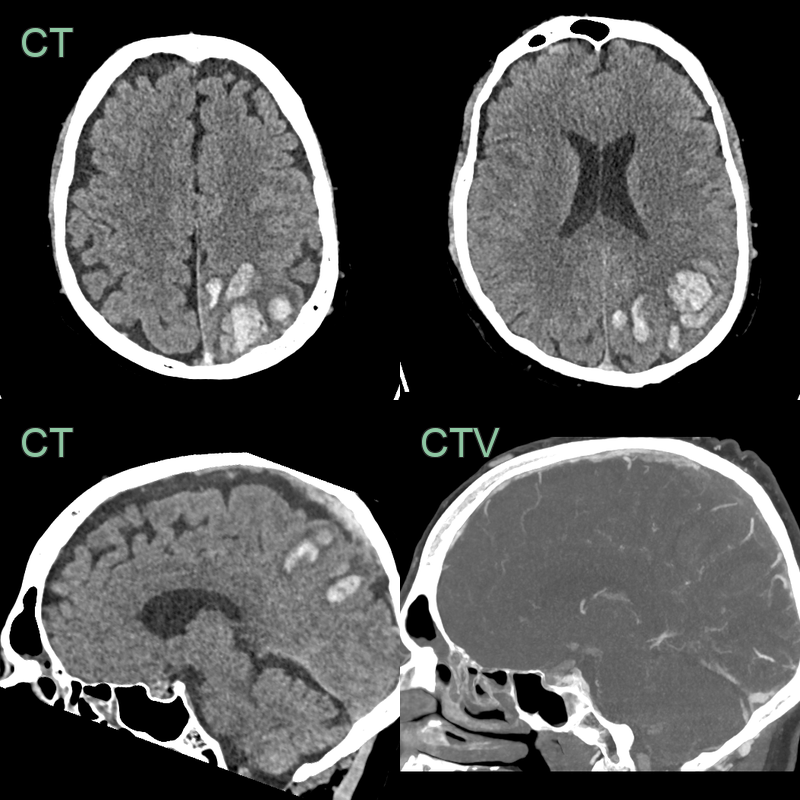
- 65-year-old patient on treatment for metastatic lung cancer.
- CT showed hyperdensity in the straight sinus, vein of Galen and internal cerebral veins.
- These vessels did not enhance on the CTV.
- MRI the next day showed hyperintensity and swelling of the deep grey structures and the capsular white matter.

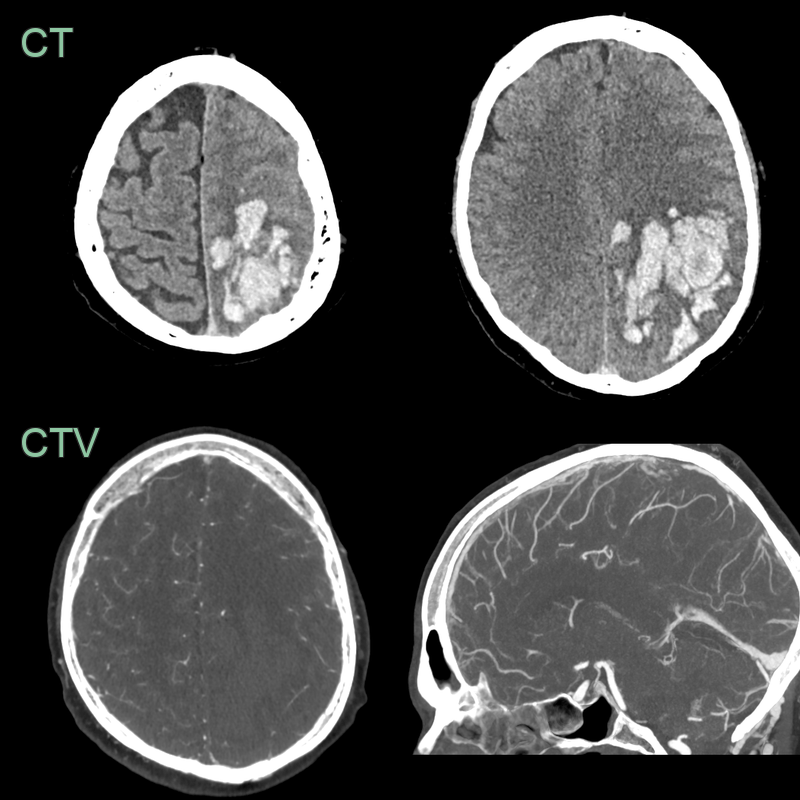
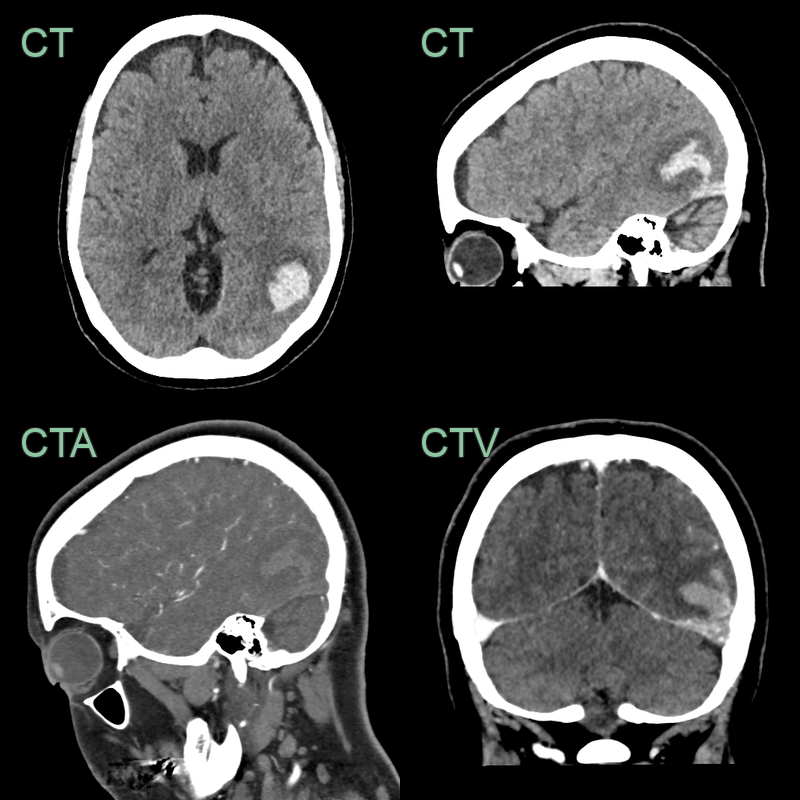
- 50-year-old patient presented with headache and dysphasia.
- CT showed a hyperdense superior sagittal sinus and a lobulated, fractionated, haematoma in the left parietal and occipital lobe.
- Despite a successful venous thrombectomy, thrombus reaccumulated in the superior sagittal sinus and the haematoma enlarged.
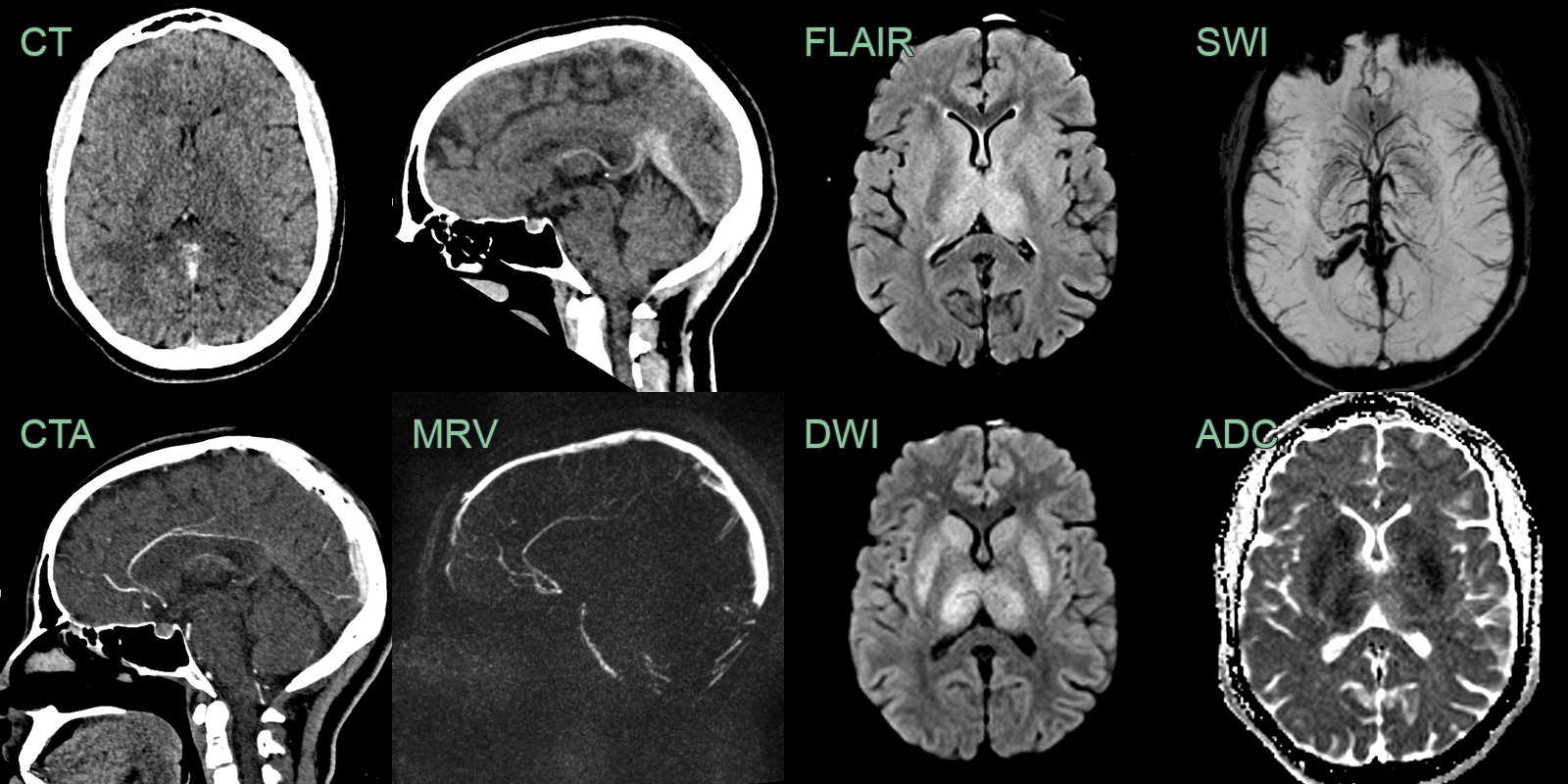
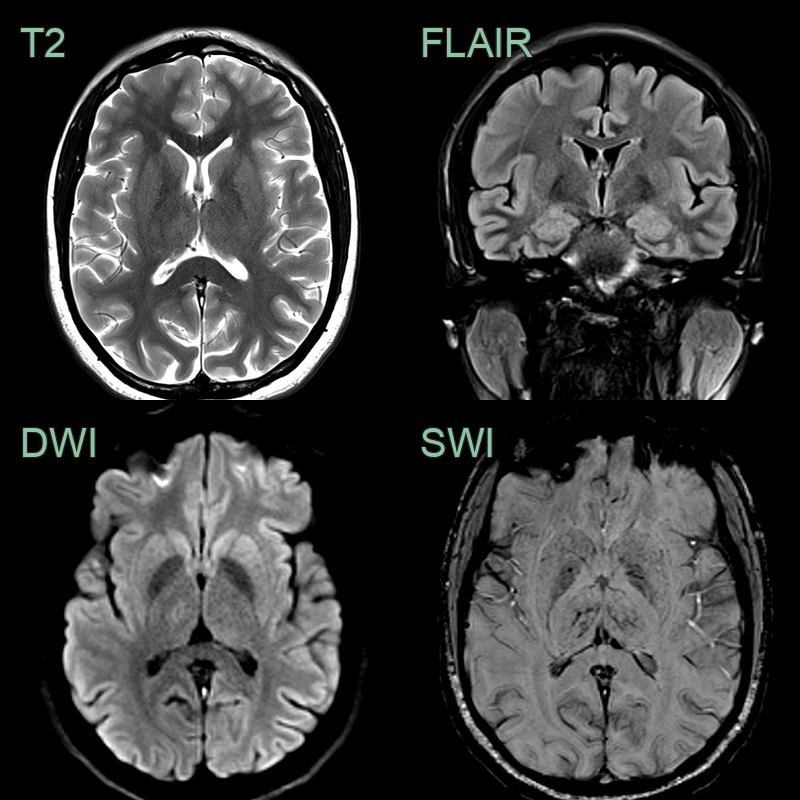
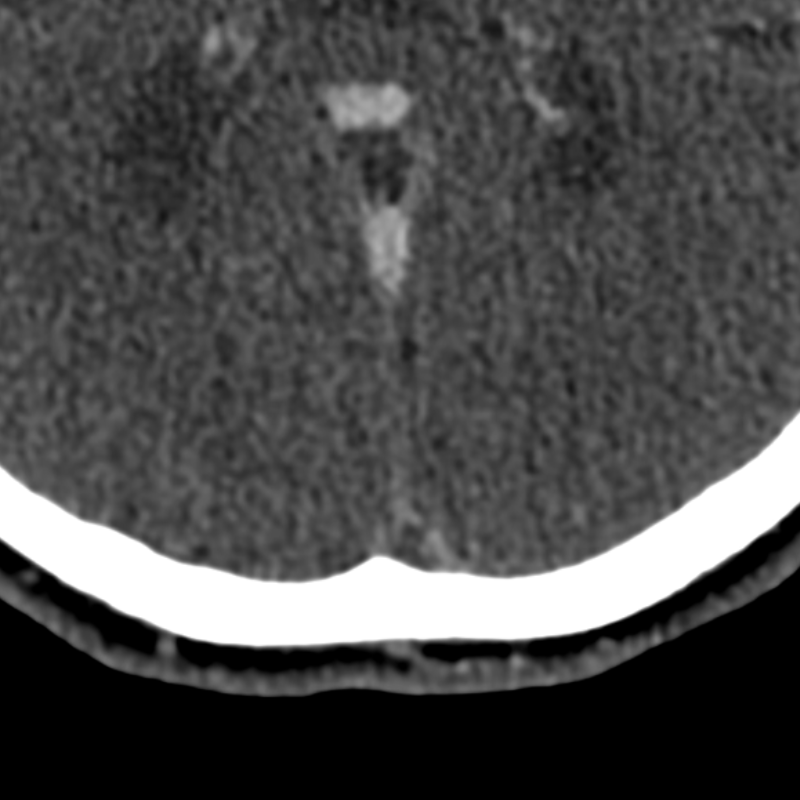
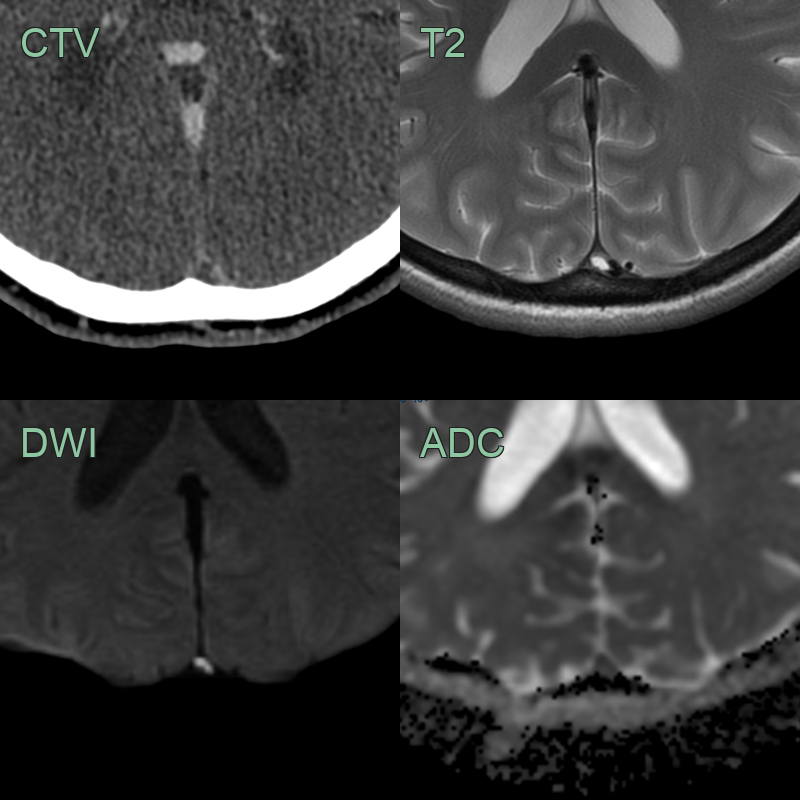
- 30-year-old patient presented with headache, confusion and expressive dysphasia.
- CT showed subtle hypodensity in the deep grey nuclei and hyperdensity within the straight sinus, vein of Galen, and internal cerebral veins. These structures were occluded on both the CTA and phase-contrast MRV.
- MRI showed hyperintensity and diffusion restriction in the deep grey nuclei. SWI showed congenstion of the deep venous system.
- 2 weeks later, a repeat MRI showed only very minimal hyperintensity in the thalami (where some microhaemorrhages had developed) indicating that the diffusion restriction was largely reversible although a few microhaemorrhages developed in the thalami.
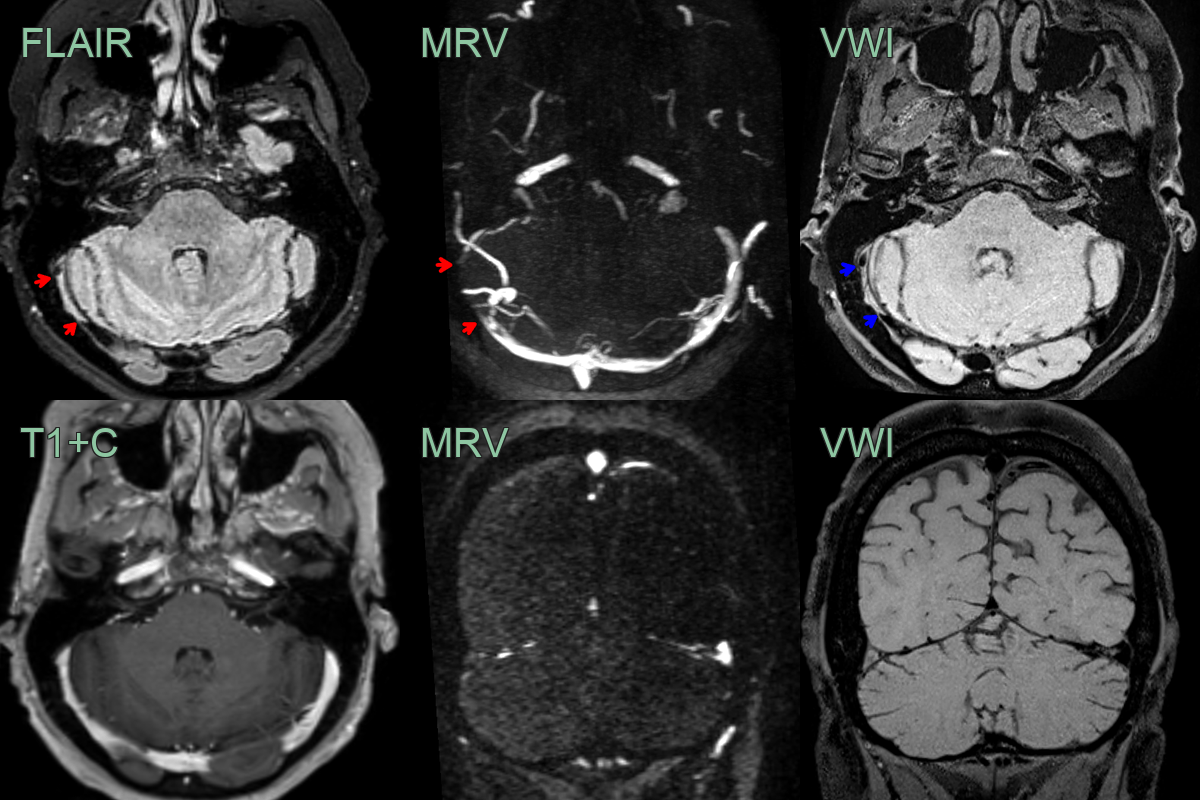
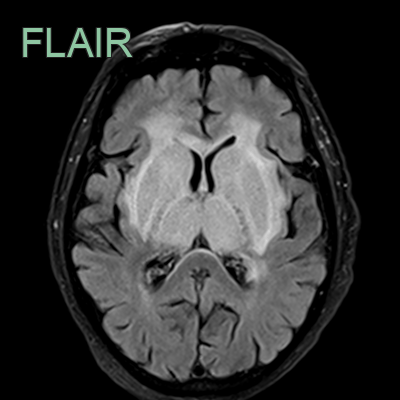
- A 35-year-old patient presented 3 months after the onset of a headache.
- FLAIR showed a hyperintense segment in the right transverse sinus with absent flow on the MRV (red arrows).
- While thrombus was strongly suspected, this was confirmed with black blood imaging (blue arrows), removing the possibility of the findings on FLAIR and MRV were artefactual.
- Notice that on the post-gadolinium images, the filling defect is not apparent due to thrombus enhancement.
Treatment¶
- Anticoagulation:
- Mainstay of treatment
- Low molecular weight heparin or unfractionated heparin, followed by oral anticoagulants
- Duration: 3-12 months, depending on underlying etiology and risk factors
- Supportive measures:
- Hydration
- Seizure prophylaxis
- Management of increased intracranial pressure
- Endovascular interventions:
- Considered in severe cases with clinical deterioration despite anticoagulation
- Options include mechanical thrombectomy and local thrombolysis
- Treatment of underlying conditions (e.g., infections, malignancy)
- Long-term follow-up:
- Neurological assessment
- Repeat imaging to evaluate recanalization
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Subarachnoid haemorrhage | Hyperdense blood in subarachnoid cisterns on CT; no sinus filling defect |
| Meningitis | Leptomeningeal enhancement on contrast MRI; no sinus filling defect; no venous territory infarct |
| Idiopathic intracranial hypertension | Patent venous sinuses on MR venography; no filling defects; may show sinus stenosis |
| Brain tumour | Focal enhancing mass with surrounding oedema; no venous occlusion; no haemorrhagic venous infarct pattern |
| Arterial ischaemic stroke | Arterial territory distribution; wedge-shaped cortical infarct; no crossing of arterial territories |
| Reversible cerebral vasoconstriction syndrome | Arterial narrowing and beading on angiography; no sinus thrombosis |
| Cerebral abscess | Smooth thin ring enhancement; restricted central DWI; no sinus filling defect |
| Subdural haematoma | Crescent-shaped extra-axial collection following brain contour; no sinus filling defect |