Dysembryoplastic Neuroepithelial Tumour (DNET)¶
Summary
- Benign, slow-growing glioneuronal tumour typically presenting with drug-resistant epilepsy in children and young adults
- Characterised by cortical location, multinodular architecture, and specific glioneuronal element
- Imaging shows a cortical-based, multicystic lesion with minimal or no enhancement
Pathophysiology¶
- Arises from abnormal development of neuroepithelial cells during embryogenesis
- Composed of oligodendrocyte-like cells, astrocytes, and floating neurons
- Typically lacks mitotic activity and necrosis
- Associated with cortical dysplasia in up to 80% of cases
Demographics¶
- Most common in children and young adults
- Mean age at diagnosis: 14-18 years
- Slight male predominance (male:female ratio 1.2:1)
- Accounts for 0.2-0.8% of all intracranial neoplasms
Diagnosis¶
- Clinical presentation:
- Drug-resistant focal epilepsy (>90% of cases)
- Seizure onset typically in childhood or adolescence
- Normal neurological examination in most patients
- Histopathology:
- WHO grade 1 tumour
- Specific glioneuronal element: oligodendrocyte-like cells arranged in columns
- Floating neurons in a mucoid matrix
- Immunohistochemistry: CD34 positivity in oligodendrocyte-like cells
Imaging¶
- CT:
- Hypodense cortical-based lesion
- Calcifications in 20-30% of cases
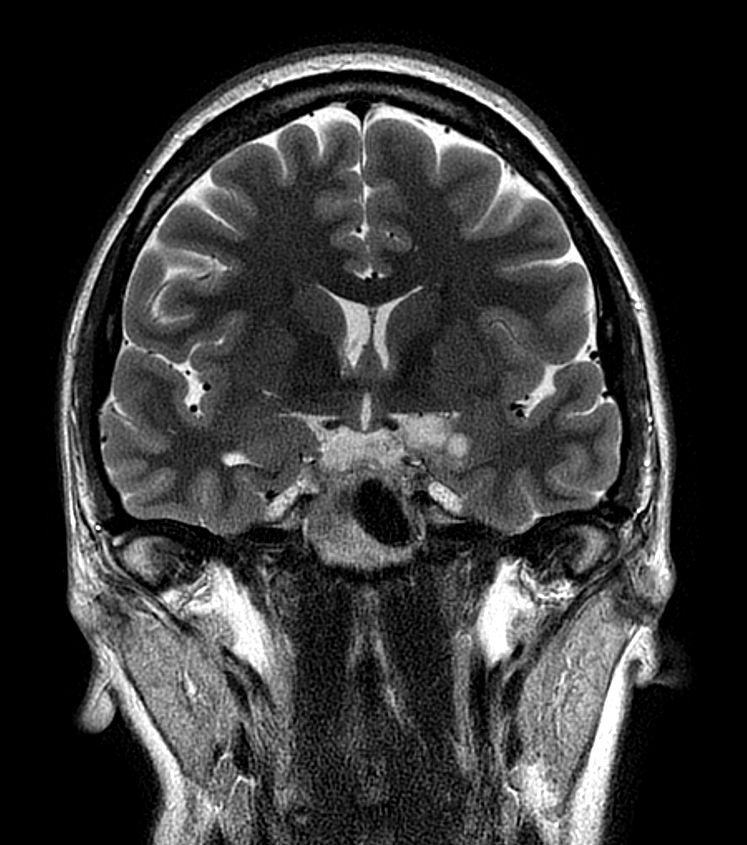
- MRI:
- T1: Hypointense to grey matter
- T2/FLAIR: Hyperintense, multicystic appearance ("bubbly" or "soap bubble" appearance)
- Minimal or no enhancement after gadolinium administration
- No perilesional oedema
- "Bright rim sign": T2 hyperintense rim at the tumour-cortex interface (specific for DNET)
- Advanced imaging:
- MR spectroscopy: Reduced N-acetylaspartate, elevated myoinositol
- Perfusion imaging: Low relative cerebral blood volume
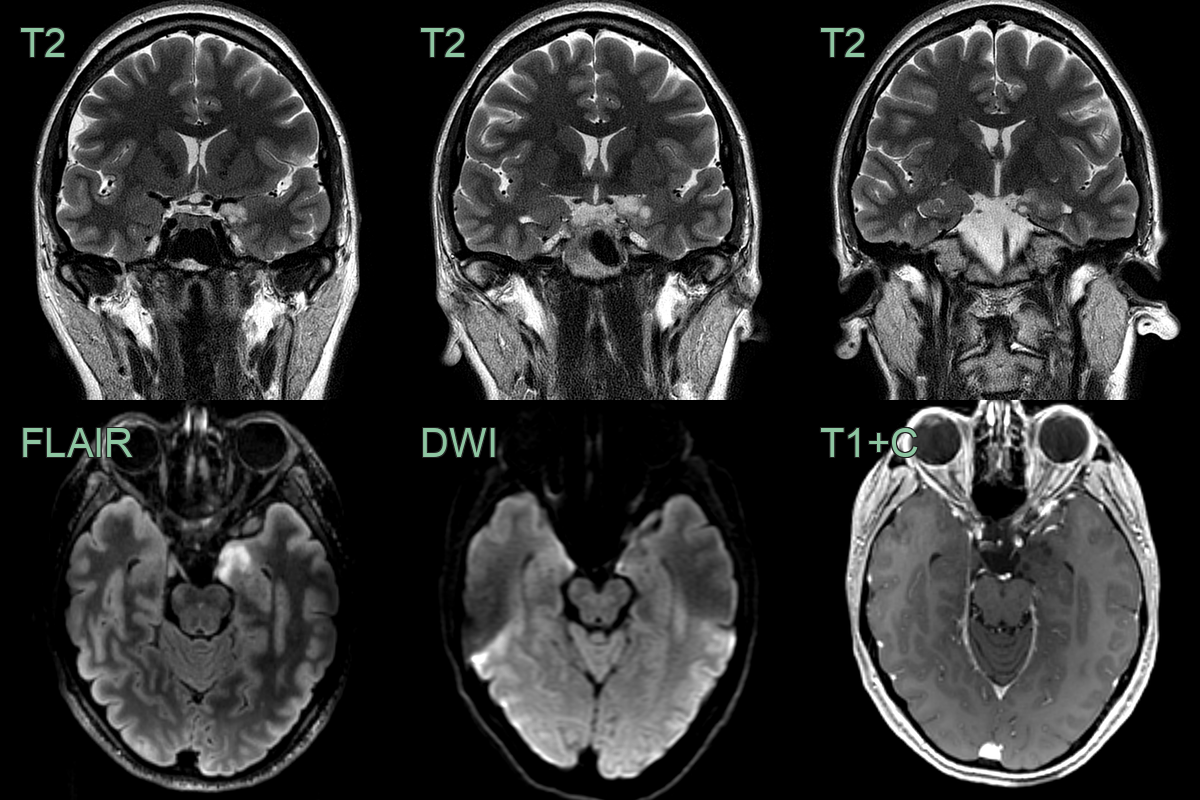
- Soap-bubble non-enhancing lesion in the left uncus has not changed in over 6 years giving a radiological diagnosis of DNET.
Treatment¶
- Surgical resection is the treatment of choice
- Complete resection achieves seizure freedom in 80-90% of cases
- Adjuvant therapy rarely required due to benign nature
- Anti-epileptic drugs for seizure control
- Long-term follow-up recommended due to rare cases of malignant transformation
- Prognosis is excellent with complete resection
- 10-year overall survival rate >90%
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Low-grade glioma | DNETs have a characteristic "bubbly" appearance on T2-weighted MRI, while low-grade gliomas typically appear more homogeneous |
| Ganglioglioma | DNETs lack the calcifications often seen in gangliogliomas on CT scans |
| Focal cortical dysplasia | DNETs have a well-defined border, while focal cortical dysplasia often has blurred gray-white matter junction |
| Oligodendroglioma | DNETs are typically located in the temporal lobe, while oligodendrogliomas are more common in the frontal lobes |
| Pleomorphic xanthoastrocytoma | DNETs do not enhance with contrast, unlike pleomorphic xanthoastrocytomas which often show strong enhancement |
| Pilocytic astrocytoma | DNETs are typically cortical, while pilocytic astrocytomas are often found in the cerebellum or optic pathways |
| Cavernous malformation | DNETs lack the characteristic "popcorn" appearance and haemosiderin rim seen in cavernous malformations on MRI |
| Glioneural tumours | DNETs have a specific "floating neuron" histological pattern, which is absent in other glioneural tumours |
| Encephalocele | DNETs do not show direct communication with the subarachnoid space, unlike encephaloceles |
| Cortical tuber (in tuberous sclerosis) | DNETs are solitary lesions, while cortical tubers are typically multiple |