Ecchordosis Physaliphora¶
Summary
- Benign, congenital, hamartomatous remnant of notochord tissue
- Typically asymptomatic, incidental finding on imaging
- Characteristic T2 hyperintense, non-enhancing retroclival lesion on MRI
Pathophysiology¶
- Remnant of embryonic notochord that fails to regress during development
- Composed of physaliphorous cells with vacuolated cytoplasm
- Usually located in the prepontine cistern, attached to the dorsum sellae or clivus
Demographics¶
- Prevalence: 0.5-2% in autopsy studies
- No gender predilection
- Can occur at any age, but more commonly identified in adults
Diagnosis¶
- Usually an incidental finding on imaging or autopsy
- Rarely symptomatic, but may cause:
- Headaches
- Cranial nerve deficits (if large enough to cause compression)
- CSF leak (if communicating with the subarachnoid space)
Imaging¶
-
MRI:
- T1: Hypointense
- T2: Markedly hyperintense
- FLAIR: Hyperintense
- No enhancement with gadolinium contrast
- Typically small (<2 cm), well-circumscribed, midline retroclival lesion
- May have a thin stalk connecting to the clivus
-
CT:
- Often not visible or seen as a subtle hypodense lesion
- May show scalloping of the dorsum sellae or clivus
-
Differential diagnosis:
- Chordoma (enhances with contrast, more aggressive appearance)
- Epidermoid cyst (restricts on diffusion-weighted imaging)
- Arachnoid cyst (follows CSF signal on all sequences)
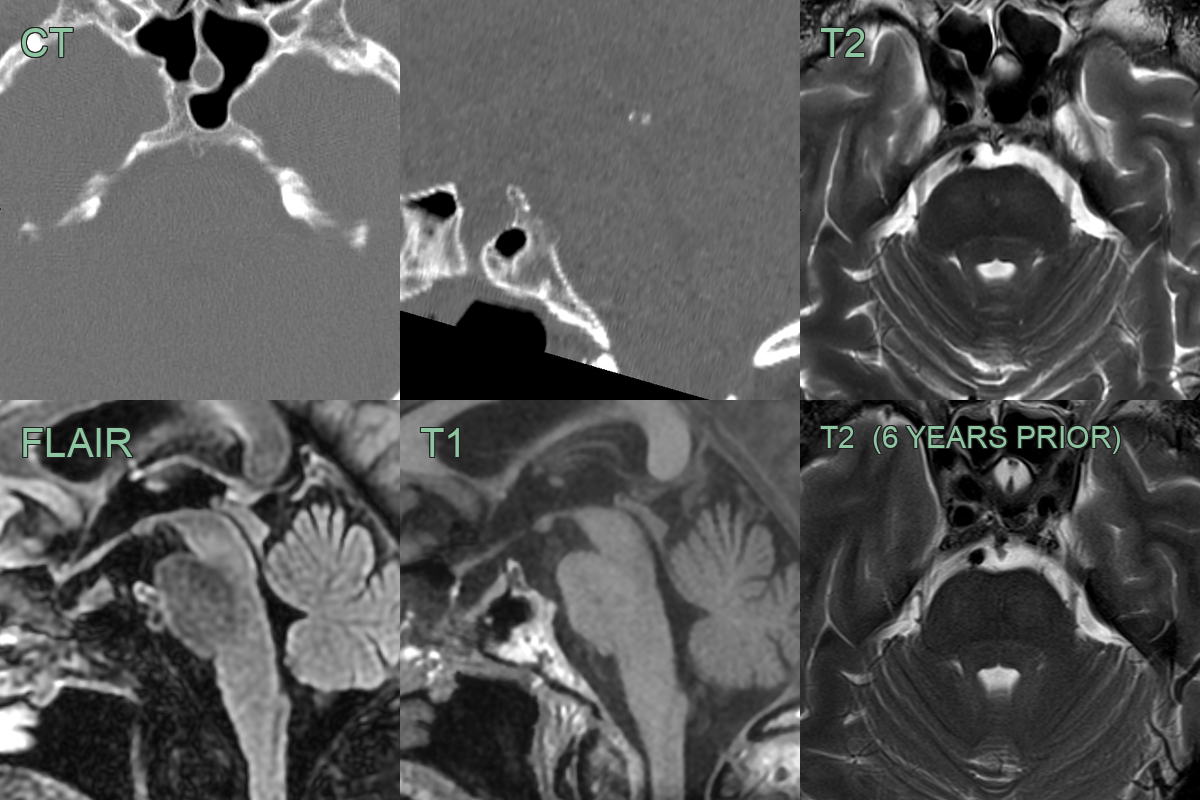
- 70-year-old male who had an MRI of the brain following a TIA.
- A bony projection arising from the clivus, associated with some exophytic soft tissue seen on FLAIR, had not changed in 6 years.
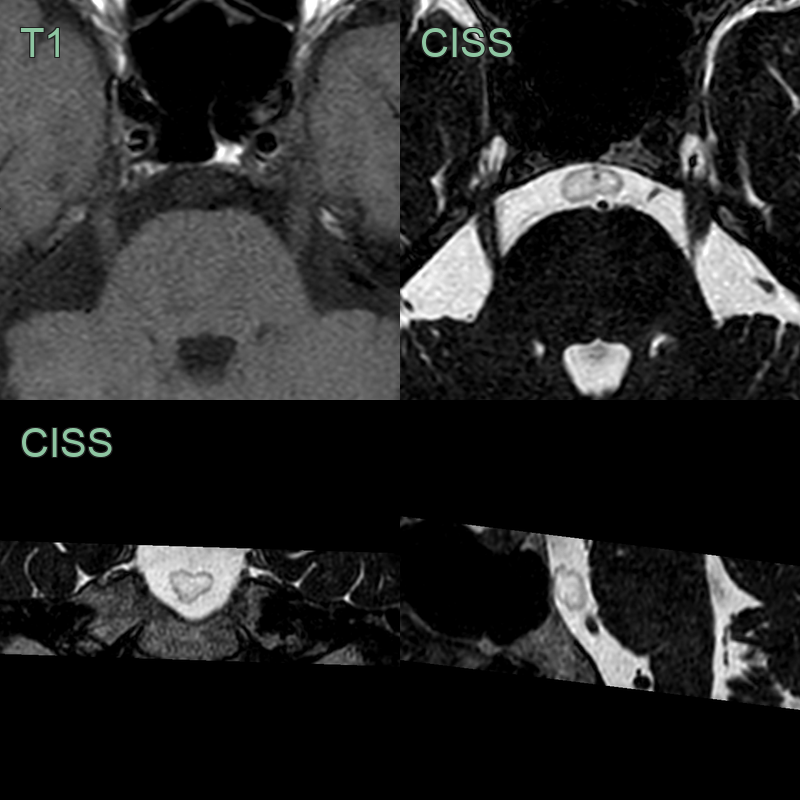
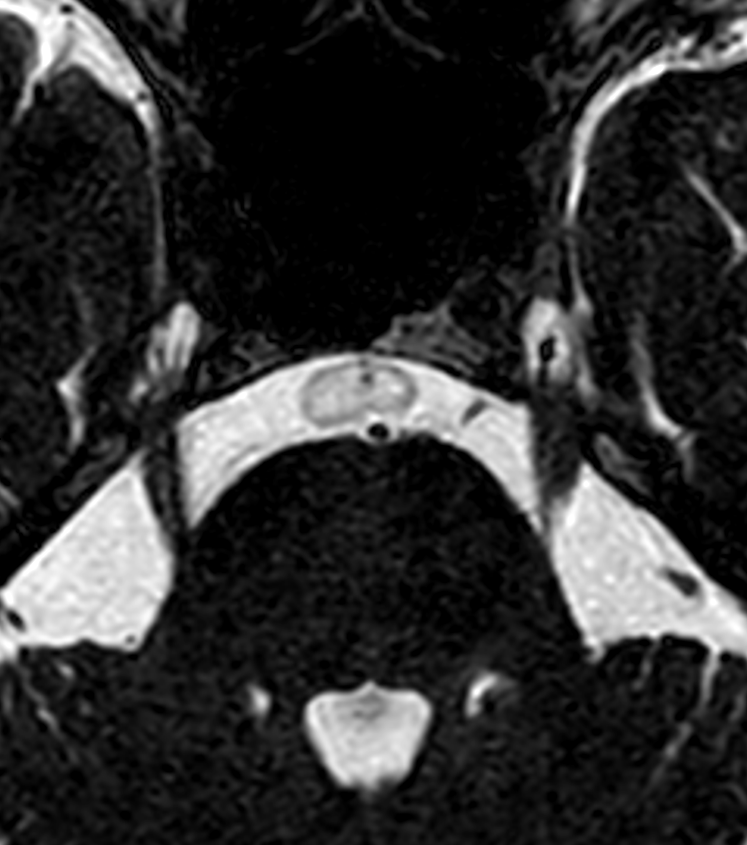
- An incidental lesion in the pre-pontine cistern was identified following an MRI for sensorineural hearing loss.
- A cystic-like lesion in the pre-pontine cistern with a focal attachment to the clivus was consistent with ecchordosis physaliphora.
Treatment¶
- No treatment required for asymptomatic lesions
- Observation with follow-up imaging to ensure stability
-
Surgical resection only considered for:
- Symptomatic lesions causing mass effect
- Lesions with progressive growth on follow-up imaging
- Cases with CSF leak
-
Biopsy generally not recommended due to:
- Risk of CSF leak
- Potential for seeding along the biopsy tract
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Chordoma | Ecchordosis physaliphora is typically smaller (<2cm) and asymptomatic, while chordomas are larger and often symptomatic |
| Chondrosarcoma | Ecchordosis physaliphora does not show bone destruction or invasion, unlike chondrosarcoma |
| Meningioma | Ecchordosis physaliphora is typically T2 hyperintense on MRI, while meningiomas are usually T2 isointense |
| Pituitary adenoma | Ecchordosis physaliphora is located in the prepontine cistern, while pituitary adenomas arise from the sella turcica |
| Epidermoid cyst | Ecchordosis physaliphora does not restrict on diffusion-weighted imaging, unlike epidermoid cysts |
| Arachnoid cyst | Ecchordosis physaliphora shows T1 hypointensity and T2 hyperintensity, while arachnoid cysts follow CSF signal on all sequences |
| Schwannoma | Ecchordosis physaliphora is midline, while schwannomas are typically eccentric and associated with cranial nerves |
| Metastasis | Ecchordosis physaliphora has a characteristic stalk connecting it to the clivus, which is not seen in metastases |