Embolic Infarcts¶
Summary
- Embolic infarcts result from occlusion of cerebral arteries by emboli originating from a distant source
- Characterised by sudden onset of neurological deficits and typical imaging findings
- Rapid diagnosis and treatment are crucial for improved patient outcomes
Pathophysiology¶
- Emboli originate from various sources:
- Cardiac (e.g., atrial fibrillation, valvular disease)
- Arterial (e.g., carotid atherosclerosis)
- Paradoxical (e.g., patent foramen ovale)
- Emboli travel through the arterial system and lodge in cerebral vessels
- Occlusion leads to ischaemia and subsequent infarction of brain tissue
- Multiple, bilateral, or scattered infarcts suggest an embolic etiology
Demographics¶
- Risk factors include:
- Advanced age
- Atrial fibrillation
- Valvular heart disease
- Atherosclerosis
- Hypercoagulable states
- Incidence increases with age
- No significant gender predilection
Diagnosis¶
- Clinical presentation:
- Sudden onset of focal neurological deficits
- Symptoms depend on the affected vascular territory
- Physical examination:
- Neurological deficits corresponding to the affected brain region
- Possible cardiac abnormalities (e.g., arrhythmias)
- Laboratory tests:
- Complete blood count
- Coagulation profile
- Lipid panel
- Cardiac evaluation:
- Electrocardiogram (ECG)
- Echocardiography (transthoracic and/or transesophageal)
- Vascular imaging:
- Carotid duplex ultrasonography
- CT or MR angiography of head and neck vessels
Imaging¶
- Computed Tomography (CT):
- Non-contrast CT:
- Hypodense areas in affected vascular territories
- May be normal in hyperacute phase (<6 hours)
- CT angiography:
- Identifies vessel occlusion and collateral circulation
- Helps determine eligibility for endovascular treatment
- Magnetic Resonance Imaging (MRI):
- Diffusion-weighted imaging (DWI):
- High sensitivity for acute infarcts
- Appears hyperintense within minutes of onset
- FLAIR sequence:
- Shows hyperintense signal in subacute and chronic stages
- Susceptibility-weighted imaging (SWI):
- Detects haemorrhagic transformation
- Typical imaging patterns:
- Wedge-shaped cortical and subcortical infarcts
- Multiple vascular territories involvement
- Bilateral or scattered distribution
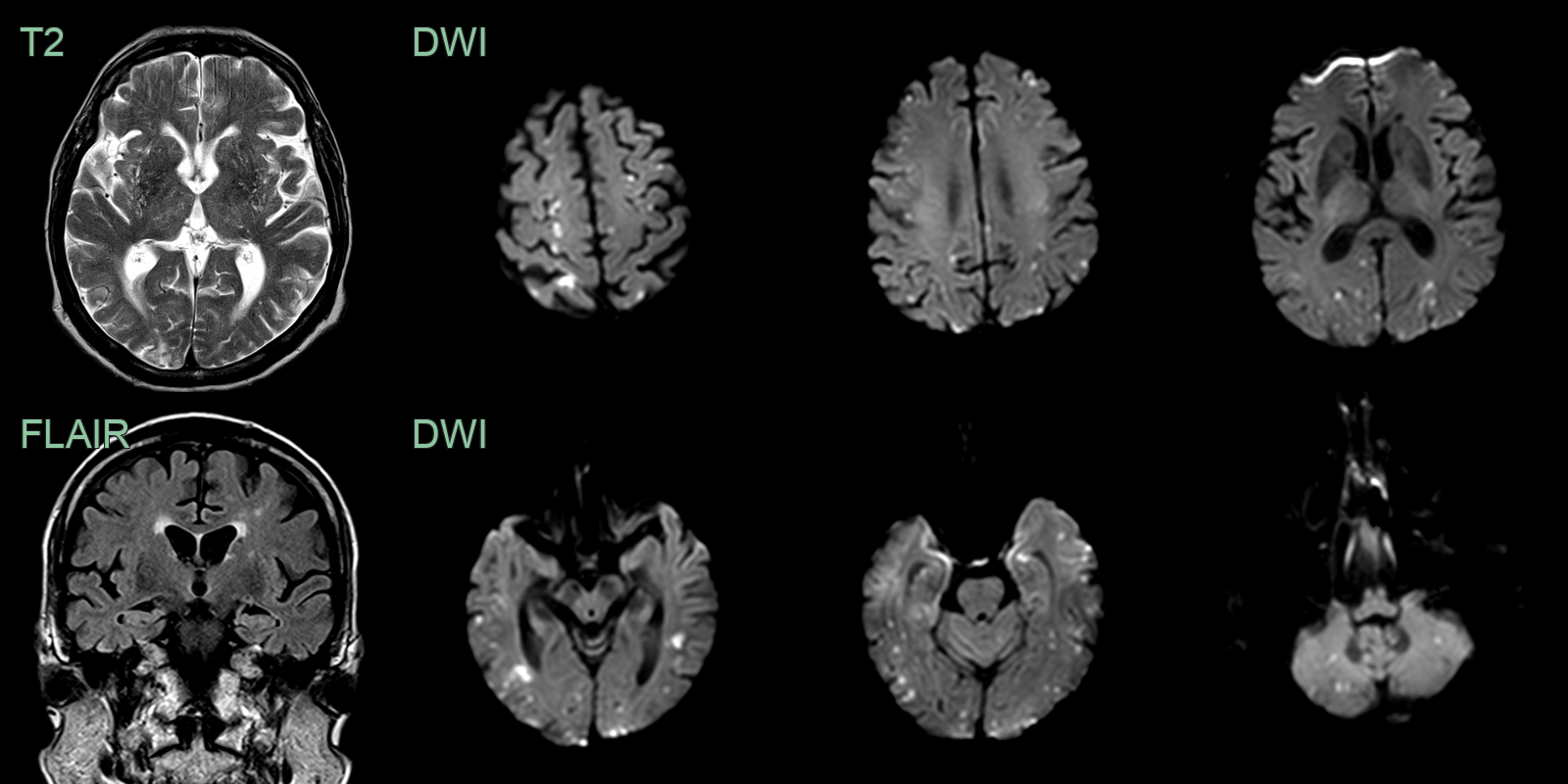
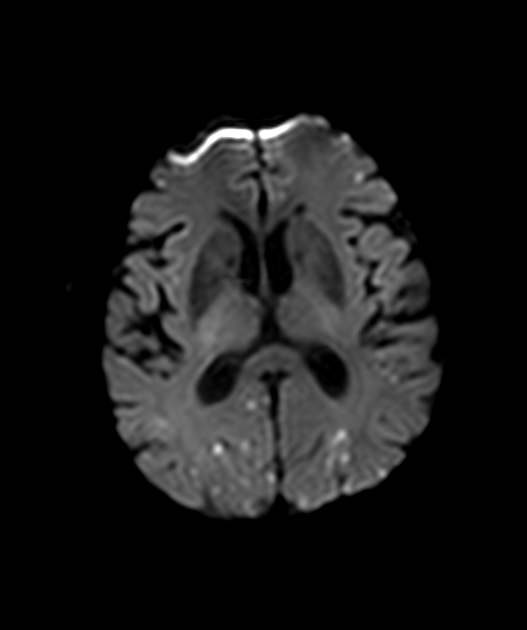
- 65-year-old patient with newly diagnosed atrial fibrillation presented with speech distrubance, left leg weakness and ataxia.
- MRI showed many scattered infarcts in both the anterior and posterior circulation.
Treatment¶
- Acute management:
- Intravenous thrombolysis with recombinant tissue plasminogen activator (rtPA)
- Within 4.5 hours of symptom onset
- Mechanical thrombectomy
- For large vessel occlusions within 6-24 hours of onset
- Secondary prevention:
- Anticoagulation for cardioembolic sources (e.g., atrial fibrillation)
- Antiplatelet therapy for non-cardioembolic sources
- Statins for atherosclerotic disease
- Management of underlying risk factors (e.g., hypertension, diabetes)
- Rehabilitation:
- Physical therapy
- Occupational therapy
- Speech and language therapy
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Thrombotic Infarcts | Often involves larger vessels, may have a more gradual onset |
| Lacunar Infarcts | Typically smaller (<1.5 cm), occur in deep brain structures |
| Haemorrhagic Stroke | Presence of blood on CT/MRI, often more severe headache |
| Brain Tumour | Mass effect, surrounding oedema, irregular borders on imaging |
| Multiple Sclerosis | Multiple white matter lesions, often periventricular |
| Transient Ischaemic Attack | Symptoms resolve within 24 hours, no permanent infarct on imaging |
| Migraine with Aura | Gradual onset, often with visual symptoms, no infarct on imaging |
| Seizure | Ictal and post-ictal symptoms, EEG abnormalities |
| Vasculitis | Multifocal infarcts, inflammatory markers elevated |
| Venous Sinus Thrombosis | Headache, often affects young adults, visible on MRV |