Encephalocele¶
Summary
- Congenital malformation characterised by protrusion of brain tissue and meninges through a defect in the skull
- Results from failure of neural tube closure during embryonic development
- Diagnosis based on clinical presentation and neuroimaging findings
Pathophysiology¶
- Occurs due to incomplete closure of the neural tube during weeks 3-4 of embryonic development
- Classified based on location:
- Occipital (most common in Western countries)
- Frontal
- Parietal
- Basal
- Associated with other neural tube defects and genetic syndromes
Demographics¶
- Incidence: 1-4 per 10,000 live births worldwide
- Higher prevalence in Southeast Asia and parts of Africa
- Risk factors:
- Maternal folate deficiency
- Genetic predisposition
- Environmental factors (e.g., certain medications, toxins)
Diagnosis¶
- Prenatal:
- Maternal serum alpha-fetoprotein screening
- Ultrasound examination
- Postnatal:
- Physical examination
- Neuroimaging (CT, MRI)
- Genetic testing to identify associated syndromes
Imaging¶
- Ultrasound:
- Anechoic or mixed echogenic mass protruding through skull defect
- Visible skull defect
- CT:
- Bony defect in skull
- Herniated brain tissue and CSF
- 3D reconstruction useful for surgical planning
- MRI:
- Gold standard for characterising encephalocele contents
- T1 and T2-weighted images to assess brain tissue and CSF
- Helps identify associated brain malformations
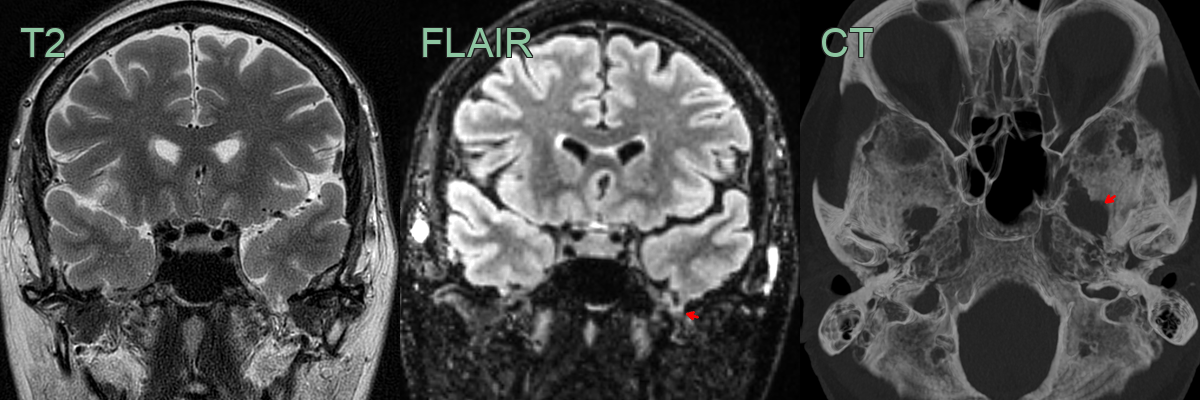
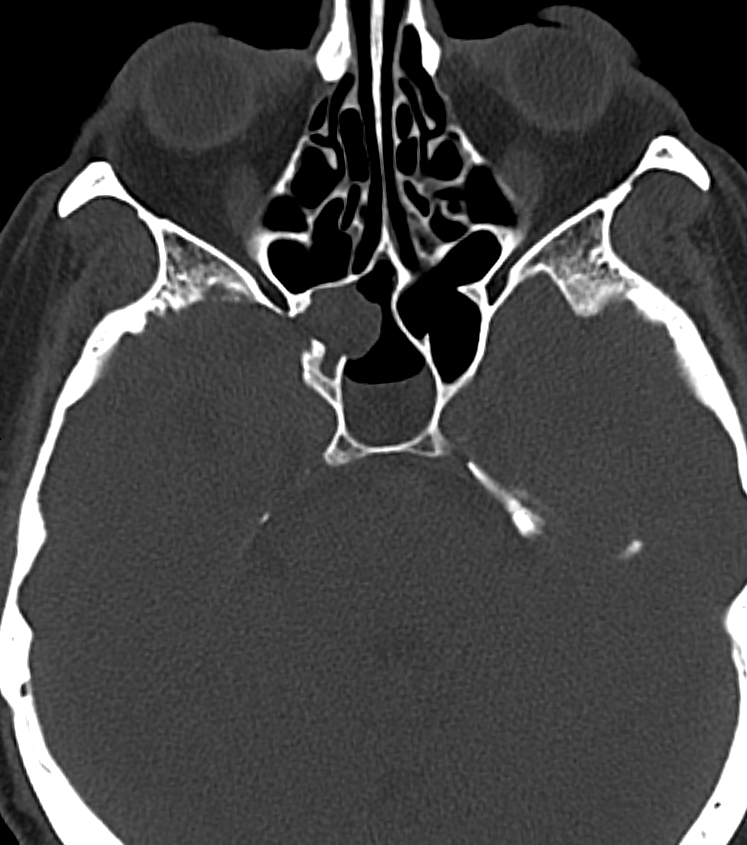
- 60-year-old patient with longterm epilepsy.
- Seizure semilogy suggesting a temporal lobe origin.
- MRI showed a small volume of the temporal lobe prolpased with T2-hyperintense gliotic signal change (red arrow).
- CT showed a defect in the skull base causing an enlarged foramen ovale.
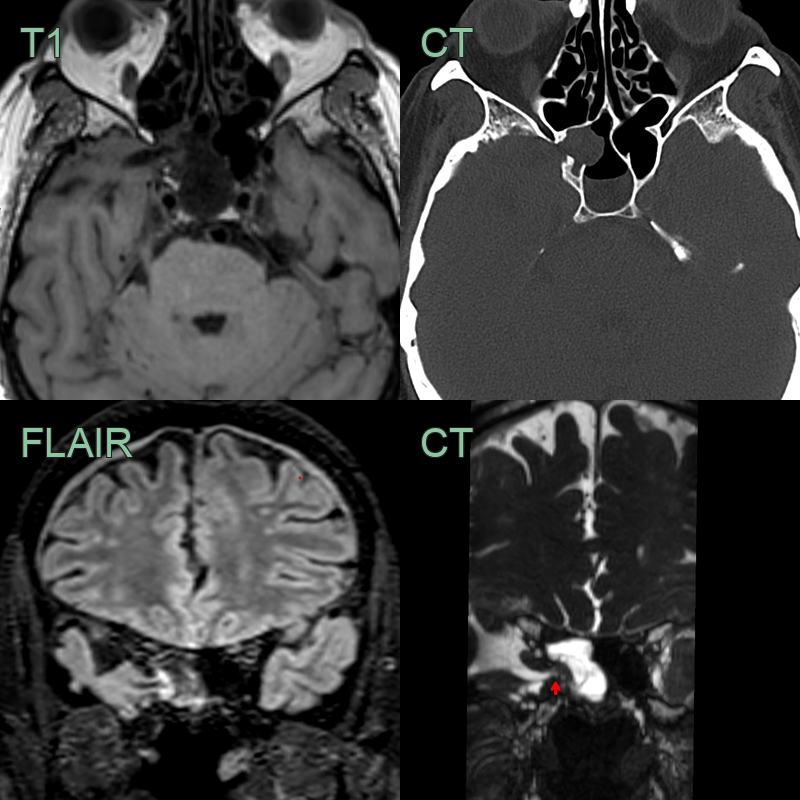
- 60-year-old patient with a longstanding nasal CSF leak.
- Medial temporal lobe encephalocele due to a defect in the lateral wall of the sphenoid bone.
- Intracranial hypotension caused shallow subdural collections.
Treatment¶
- Surgical repair:
- Typically performed in early infancy
- Goals: closure of defect, preservation of functional neural tissue
- Multidisciplinary approach:
- Neurosurgery
- Plastic surgery
- Paediatric neurology
- Rehabilitation services
- Long-term follow-up:
- Monitoring for hydrocephalus
- Developmental assessment
- Management of associated complications (e.g., seizures, visual impairment)
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Cephalohaematoma | Doesn't cross suture lines; fluctuant swelling |
| Sinus pericranii | Reduces with pressure or in recumbent position |
| Dermoid cyst | Typically midline; doesn't transilluminate |
| Meningocele | No brain tissue within the sac |
| Atretic encephalocele | Smaller, skin-covered lesion without CSF |
| Nasal glioma | Solid mass, doesn't change size with crying |
| Teratoma | Complex mass with mixed tissue types on imaging |
| Skull fracture | History of trauma; linear lucency on X-ray |
| Langerhans cell histiocytosis | Lytic bone lesions on imaging |
| Congenital hemangioma | Vascular lesion with flow on Doppler ultrasound |